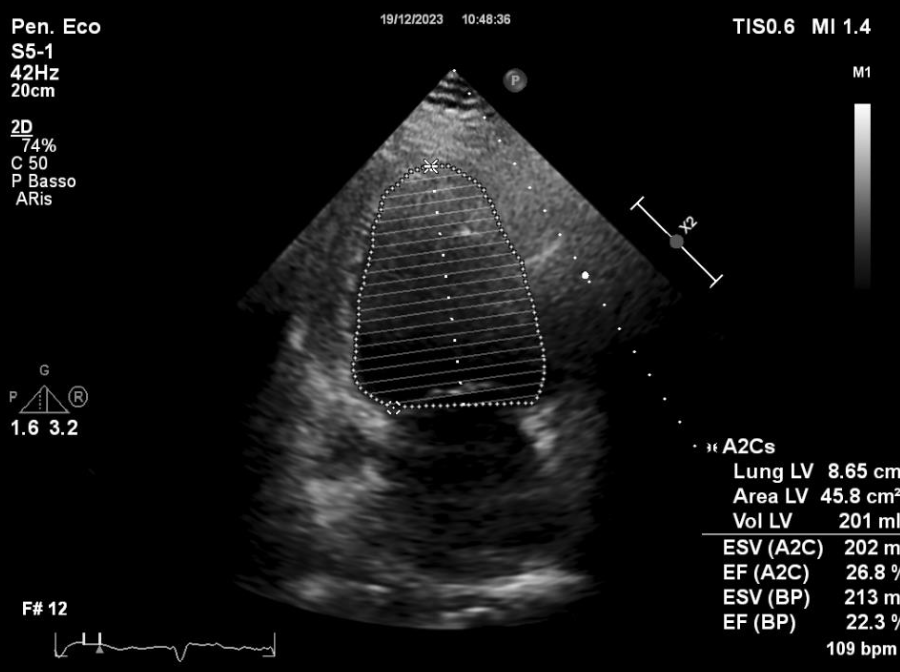
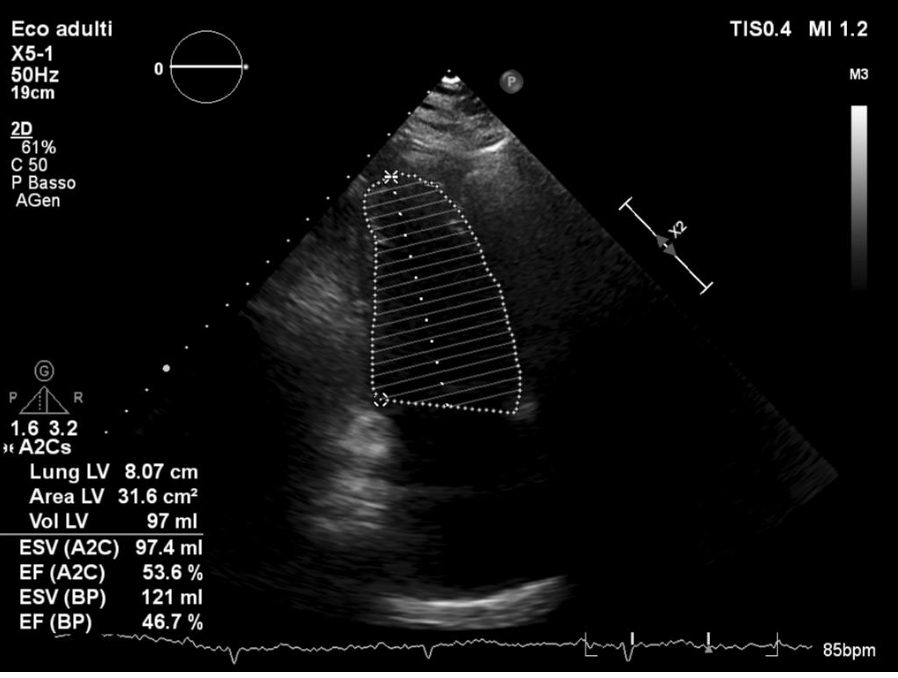
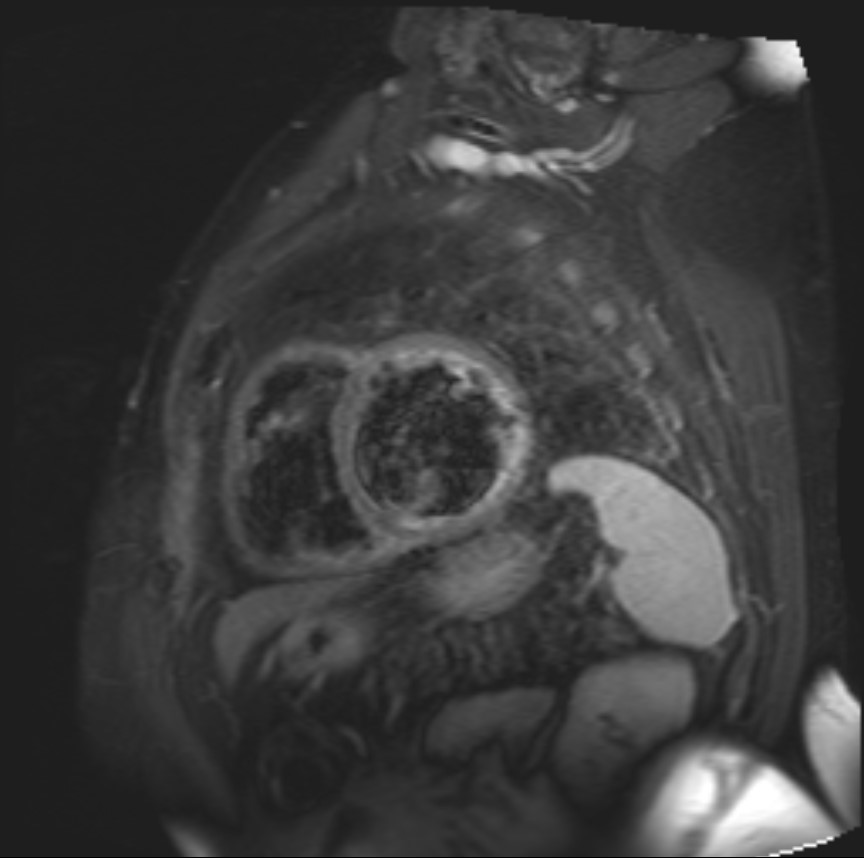
We present the clinical case of a 70-year-old male patient with multiple cardiovascular risk factors and no previous cardiac history. The first admission to our institution was in December 2023 for heart failure with reduced ejection fraction (LVEF 20–25%) with coronary arteries without critical stenoses and atrial fibrillation (AF) with moderate-to-high ventricular response. Electrical cardioversion was performed, with early recurrence of atrial fibrillation. The patient was subsequently followed at our cardiology day hospital, where he underwent multiple visits for therapeutic optimization, with poor hemodynamic stability requiring high doses of oral and intravenous diuretics. In April 2024, a further electrical cardioversion (ECV) was scheduled but not performed due to a suspected finding on transesophageal echocardiography (TEE) suggestive of intracavitary thrombosis. In October 2024, the patient was readmitted for congestive heart failure and treated with high-dose diuretics and levosimendan. In this setting, cardiac MRI revealed subendocardial late gadolinium enhancement (LGE) of the basal anteroseptal wall of the left ventricle and mid-wall LGE of the basal interventricular septum. Intracavitary thrombosis was excluded on follow-up TEE, CRT-D was implanted for primary prevention, and subsequent ECV was acutely effective in restoring sinus rhythm. After hemodynamic optimization, the patient was rehospitalized in January 2025 and he underwent ablation of the cavotricuspid isthmus and circumferential pulmonary vein isolation, followed by recurrence of AF at discharge. Hemodynamic compensation did not improve due to persistence of atrial fibrillation until February 2025, when sinus rhythm was documented; therefore, the CRT-D was reprogrammed to DDD mode, 40–110 bpm. At subsequent follow-ups, the patient consistently remained in sinus rhythm, with progressive improvement in dyspnea (NYHA class I–IIa), circulatory compensation, and left ventricular function. At the most recent transthoracic echocardiogram (July 2025), LVEF was 47%, with diffuse hypokinesia, severely dilatated left ventricle, dilated atria and mild mitral regurgitation. This clinical case highlights how the ablation of cavotricuspid isthmus and circumferential pulmonary vein isolation in patients with hypokinetic–dilated cardiomyopathy and biventricular dysfunction can result in a marked and sustained improvement in ventricular function, clinical symptoms and overall prognosis.