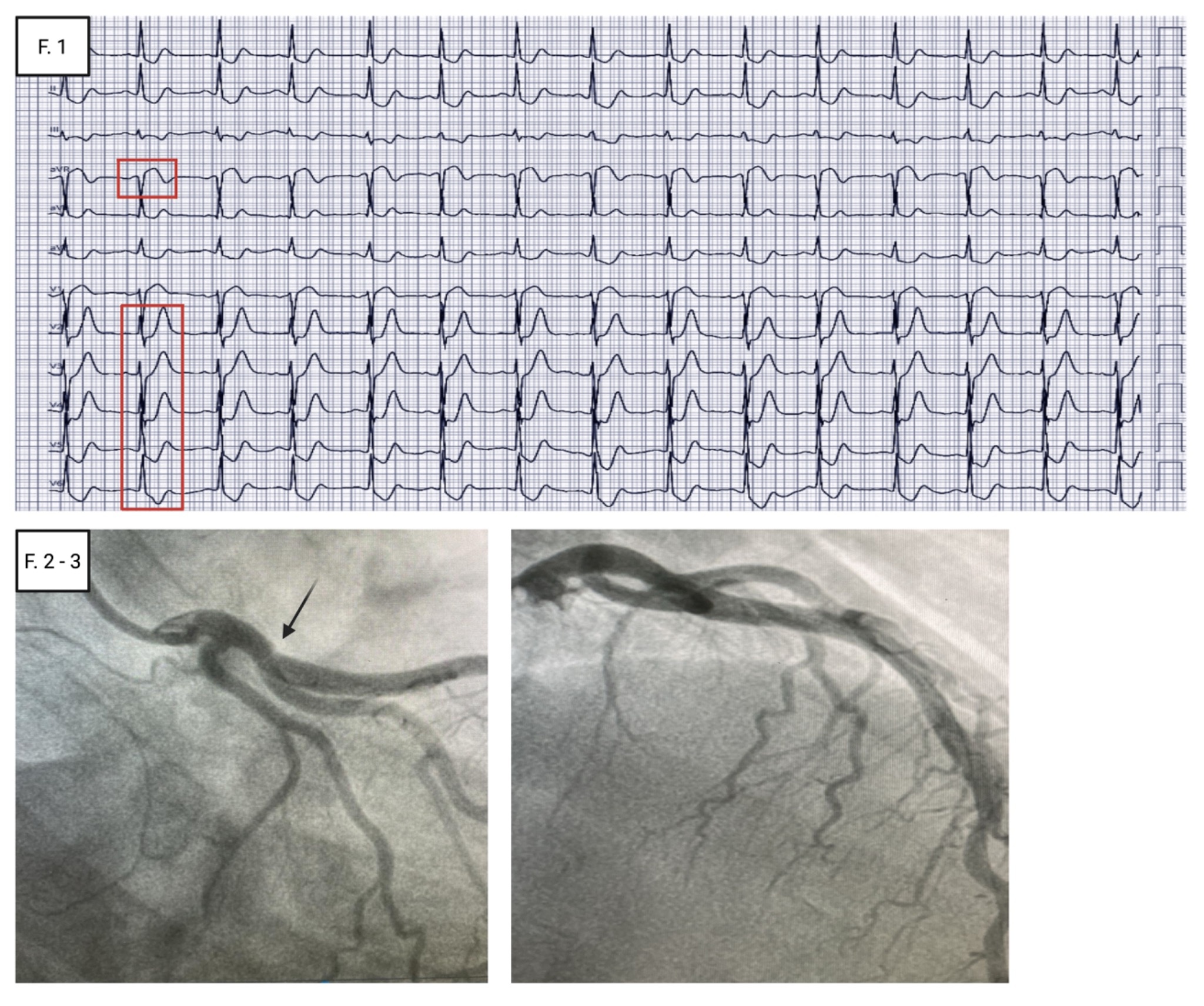
A 44-year-old woman of sub-Saharan origin presented to the Emergency Department with intermittent, oppressive, radiating chest pain unresponsive to nitrates. She had no prior cardiovascular history; multiple spontaneous miscarriages. The 12-lead ECG showed sinus tachycardia with tall, symmetric hyperacute T waves in V2–V4 accompanied by upsloping ST-segment depression. Mild ST-segment elevation was present in aVR and V1, with widespread downsloping ST depression in the remaining leads—features consistent with a de Winter pattern (Fig. 1), a STEMI equivalent, suggestive of occlusive myocardial infarction (OMI). Laboratory testing was unremarkable except for an elevation in high-sensitivity troponin I above the 99th percentile upper reference limit. Urgent transthoracic echocardiography demonstrated a non-dilated left ventricle with moderately reduced systolic function (LVEF 45%), driven by hypokinesia of the mid-to-apical interventricular septum and the anterior apex, with no significant valvular disease and no signs of central congestion. The patient was managed as a high-risk NSTEMI and underwent urgent coronary angiography, which revealed a flow-limiting spontaneous coronary artery dissection (type 2B) involving the proximal LAD–first diagonal bifurcation. Direct implantation of a single drug-eluting stent achieved an excellent final angiographic result. The in-hospital course was uncomplicated, with recovery of global and regional left ventricular function, and she was discharged on dual antiplatelet therapy on the fourth day. The de Winter pattern accounts for ~2% of acute LAD occlusions, rarely in SCAD-related events. Diagnostic criteria comprise hyperacute, symmetric precordial T waves with >1 mm upsloping ST-segment depression in V2–V6, absence of anterior ST elevation, and 0.5–1 mm ST elevation in aVR. These features reflect a proximal ischaemic injury vector directed away from the anterior precordial leads, producing reciprocal ST depression with prominent T waves, while the concomitant ST elevation in aVR represents its projection toward the right–superior quadrant, consistent with a large, proximal ischaemic territory. This case underscores that de Winter is a time-critical STEMI equivalent (OMI) and highlights SCAD as an important mechanism in young women; prompt recognition should trigger an immediate invasive pathway to mitigate adverse short- and long-term outcomes in these situations.