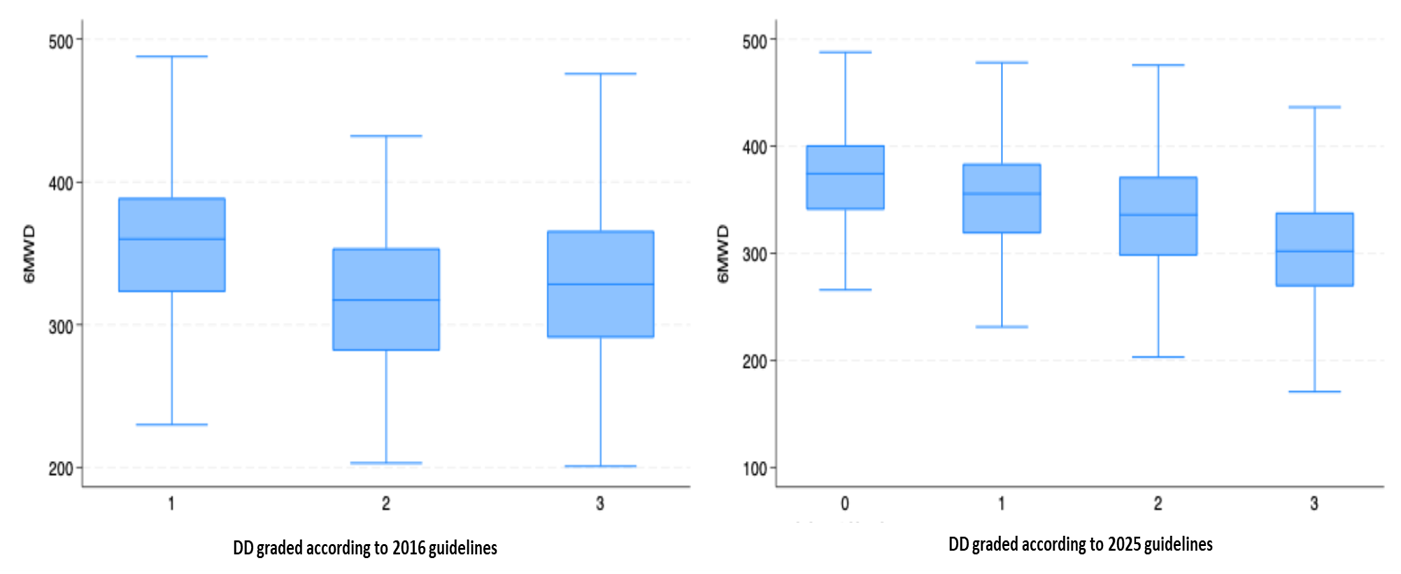
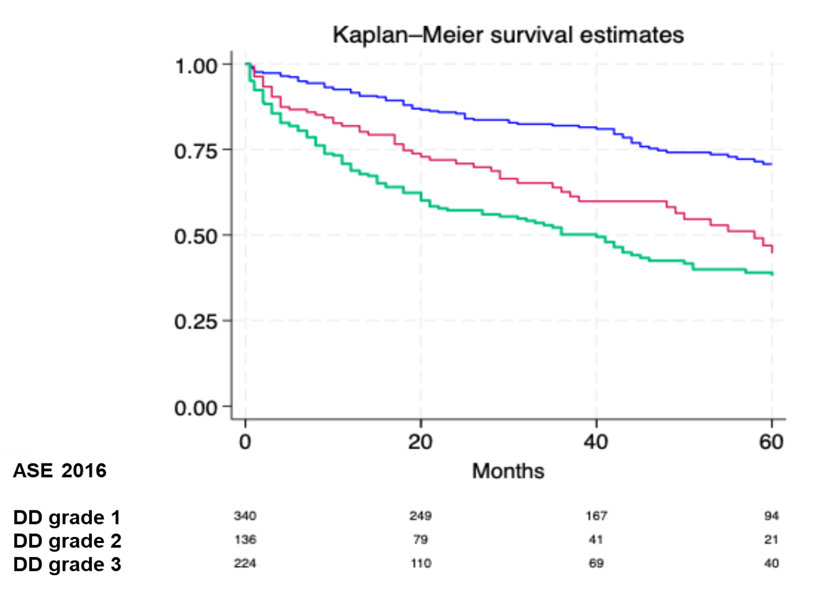
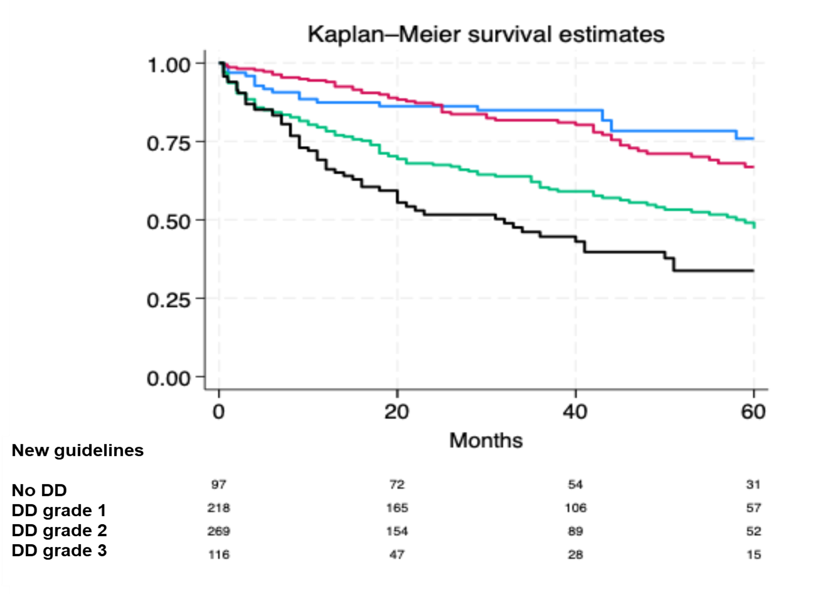
BACKGROUND: Novel guidelines for assessing diastolic dysfunction (DD) have recently been published by the American Society of Echocardiography (ASE). Their concordance with prior recommendations and potential clinical advantage remain unclear, particularly in patients with heart failure with reduced ejection fraction (HFrEF). This study aimed to test the concordance between new and previous guidelines and evaluate the clinical utility of the new criteria. METHODS: DD was assessed in 700 stable HFrEF outpatients at our institution using both the 2016 ASE guidelines and the newly published recommendations. Functional capacity was evaluated with six-minute walk test at the time of echocardiography. Associations between DD and functional capacity were tested by comparing walking distance across DD grades. Concordance between DD classifications was analyzed with kappa statistics. The primary endpoint was a composite of heart failure hospitalization and all-cause mortality. Multivariable Cox regression analyses tested the prognostic impact of DD graded according to the new guidelines. RESULTS: The median age of the cohort was 66 ± 13 years, and 74% were male. By 2016 criteria, all patients had DD (49% grade 1, 19% grade 2, 32% grade 3). With the new guidelines, 14% had no DD, while 31% had grade 1, 27% grade 2, and 17% grade 3. Concordance between DD classifications was weak (κ = 0.30). Patients with more advanced DD per the new guidelines were older, more often male, more symptomatic, on higher loop diuretic doses, and had higher NT-proBNP. Functional capacity (i.e. 6-min walking distance) did not differ across all grades with the 2016 DD criteria, but showed significant differences with DD classified according to the new guidelines (Figure). In the 33% whose DD classification were discordant, the old criteria failed to discriminate functional capacity, whereas the new classification did. Both systems stratified prognosis, with more advanced DD grades being independently associated with higher risk of the composite endpoint. CONCLUSIONS: The new ASE DD guidelines showed weak concordance with the 2016 criteria but better discriminated functional capacity and symptom burden. Both predicted prognosis, with the novel guidelines offering potentially greater clinical utility in HFrEF.