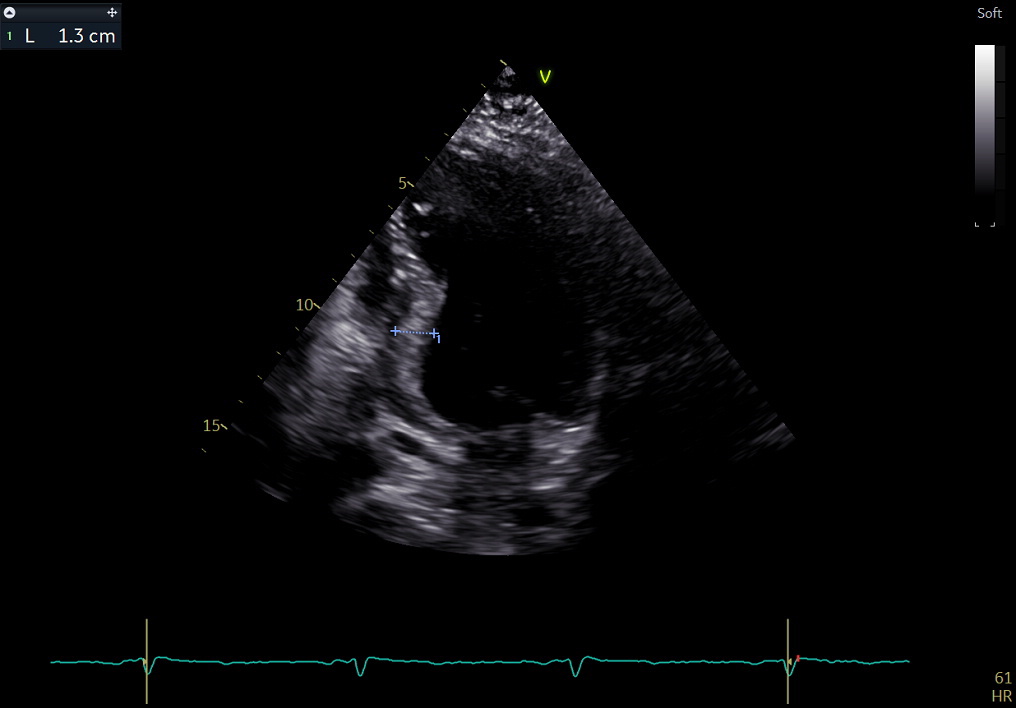
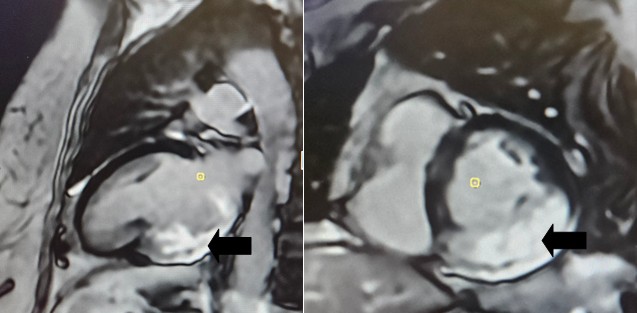
Intro: Hypertrophic cardiomyopathy (HCM) is defined by an increased left ventricular (LV) wall thickness (≥15 mm) that cannot be explained solely by abnormal loading conditions. Hypertrophy preferentially involves the basal segments of the interventricular septum, it frequently extends to the lateral wall, posterior septum, and the LV apex. Isolated lateral or inferoseptal hypertrophy are considered rare variants, pure or dominant inferior wall involvement is extremely sporadic. Hypertrophy of atypical segments may be overlooked by transthoracic echocardiography and can be difficult to differentiate from intracardiac masses; therefore, advanced diagnostic imaging, such as Cardiac Magnetic Resonance (CMR), is often required.In this article, we report a highly unusual case of isolated inferior hypertrophic cardiomyopathy. Description : A 64-year-old obese Caucasian female, with no family history of heart disease or sudden cardiac death and no prior diagnosis of hypertension, presented to the Emergency Department with palpitations and lipothymia. EKG revealed a wide-complex tachycardia at a rate of 240 bpm, likely of ventricular origin, which was successfully treated with electrical cardioversion. Bedside echocardiography showed (Fig.1) a left ventricle of normal diameter with hypo-akinesia of the mid-basal inferior wall and mildly depressed global contractility. Subsequent coronary angiography showed no evidence of significant obstructive lesions.The patient then underwent CMR, which yielded the unexpected finding of isolated involvement of the mid-basal inferior LV wall, characterized by: a) Marked hypertrophy (wall thickness of 18 mm); b) Hypo-akinesia with a mild reduction in global contractility; c) Subendocardial late gadolinium enhancement (LGE) during the perfusion study; d) Substantially transmural hyperintensity on Late Gadolinium Enhancement (LGE) imaging for fibrosis assessment (Fig. 2); e) Increased T1 mapping values (1098 ms, compared to < 994 ms in the remaining myocardium). The examination was diagnostic for hypertrophic cardiomyopathy localized to the mid-basal inferior wall of the left ventricle. Consequently, the patient underwent implantable cardioverter-defibrillator (ICD) placement. Discussion : This case of hypertrophic cardiomyopathy is unique due to the atypical and focal nature of the affected site. In this clinical scenario, Cardiac Magnetic Resonance plays a diagnostic pivotal role.