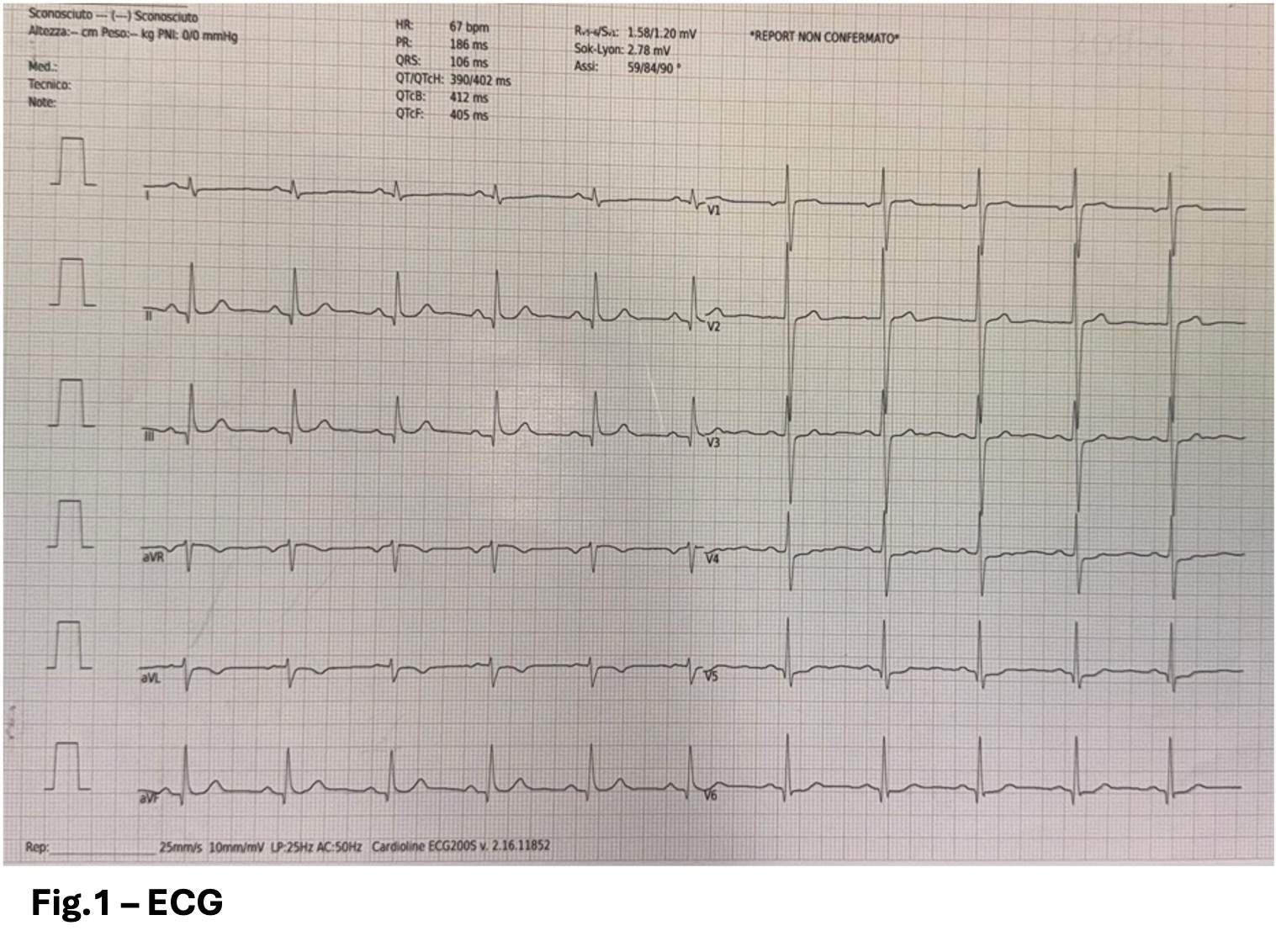
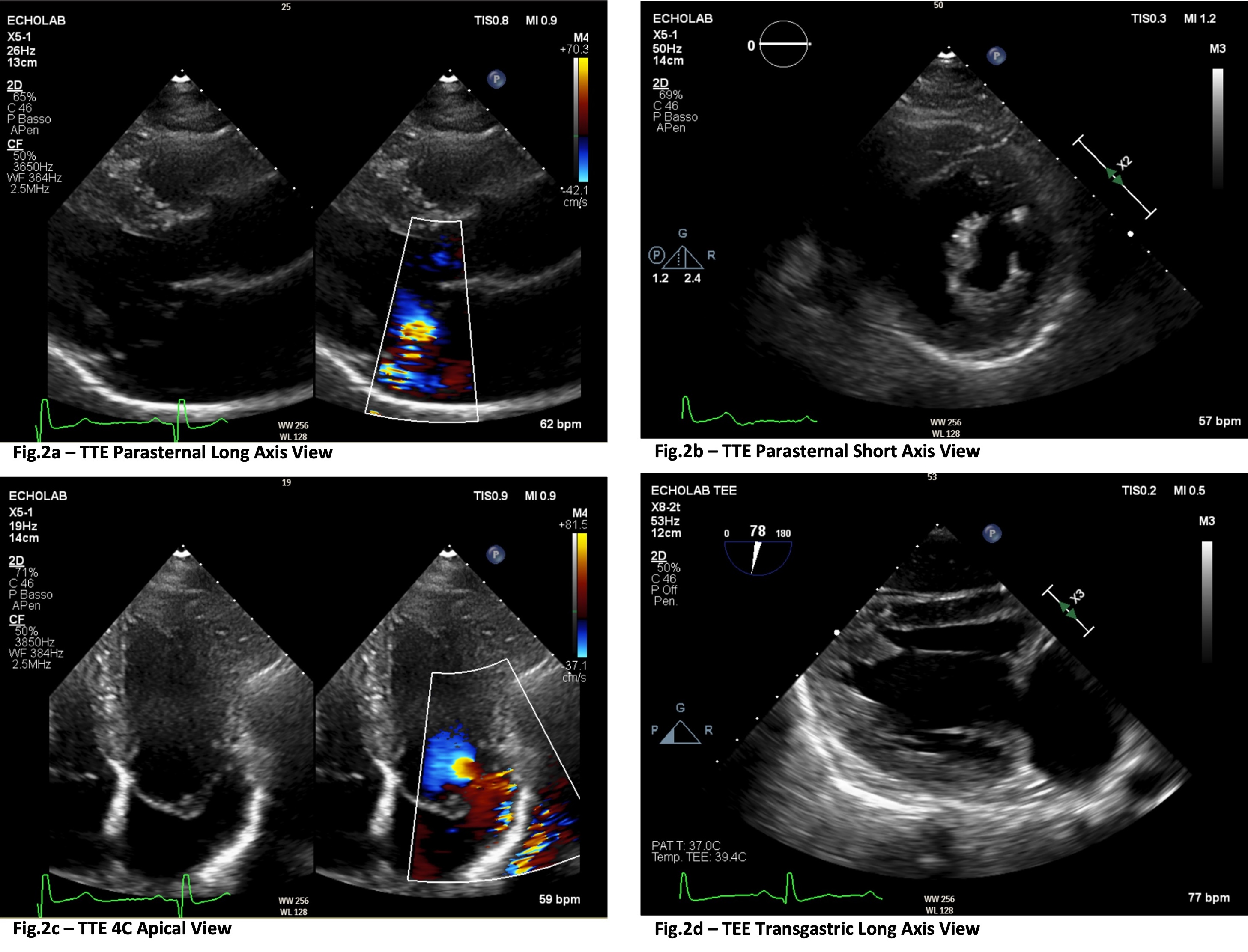
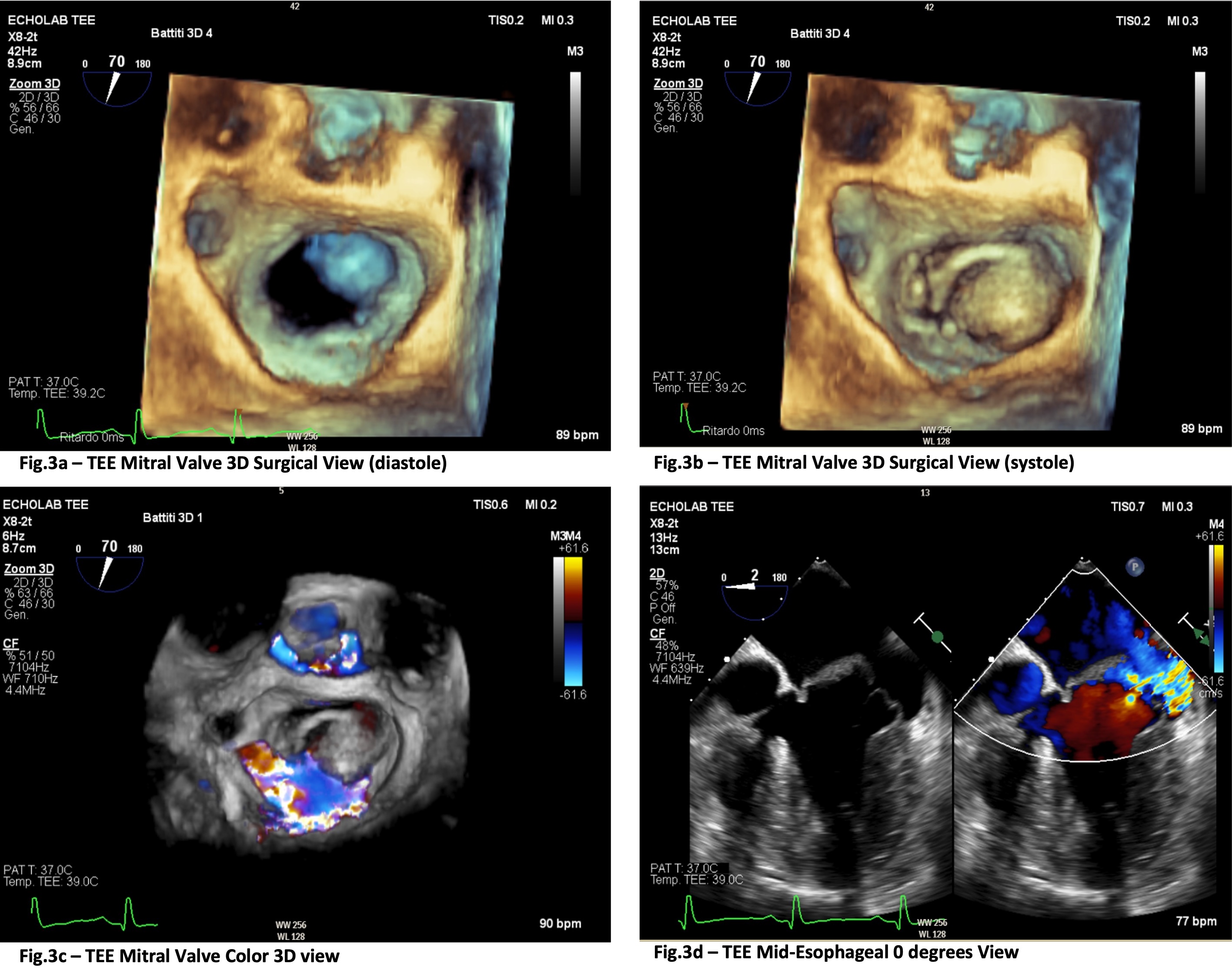
A 58-year-old man was diagnosed in his 30s with mitral valve prolapse due to myxomatous degeneration. His family history was notable for ischemic heart disease (his father died suddenly from myocardial infarction) and hypertrophic cardiomyopathy (HCM). The patient is heterozygous for a likely pathogenic variant in the troponin I gene (TNNI3), c.592C>G p.(Leu198Val), also expressed by his brother and nephews, all affected by HCM. He had no significant comorbidities. ECG showed non-significant Q waves in the inferior leads and V6, mild LV strain pattern in the lateral leads with negative T waves in aVL (Fig.1). CMR didn’t reveal any abnormalities (normal thickness, no LGE), and no arrhythmias were documented during the years. Patient underwent periodic follow-up showing abnormal features of the mitral valve apparatus: marked anterior displacement of the anterolateral commissure and posterior displacement of the posteromedial one, resulting in a ‘right-to-left’ rather than anteroposterior leaflet orientation (Fig.2b). Both papillary muscles appeared hypoplastic and were displaced apically and anteriorly (Fig.2d). There was pronounced elongation of the chordae tendineae and of the anterior mitral valve leaflet (AMVL), which was also thickened (Fig.2c). Additional findings included myxomatous degeneration of the leaflets, annular dilation with fibrosis of the posterior part and mild posterior annular curling, without significant mitral annular disjunction (Fig.2a). At most recent assessment, TTE revealed moderate-to-severe mitral regurgitation, a normal-sized left ventricle with normal wall thickness and preserved systolic function, increased filling pressure, reduced lateral e’ 4 cm/sec and medial e’ 5 cm/sec, severe left atrial enlargement, right ventricle normal in size and systolic function and normal systolic pulmonary artery pressure at rest. TEE confirmed severe mitral regurgitation with an eccentric jet (Fig.3d), originating at the A2M2/P2M2-A3/P3 segments (Fig.3c) and directed toward the posterolateral wall of the left atrium, secondary to prolapse of the AMVL (Fig.3a-b). The patient was deemed suitable and then scheduled for surgery. The ECG and echocardiographic findings are not consistent with hypertrophic cardiomyopathy. Abnormalities of the mitral valve apparatus, although showing anterior displacement of the papillary muscles and increased AMVL length, are not fully representative of ancillary manifestations of HCM.