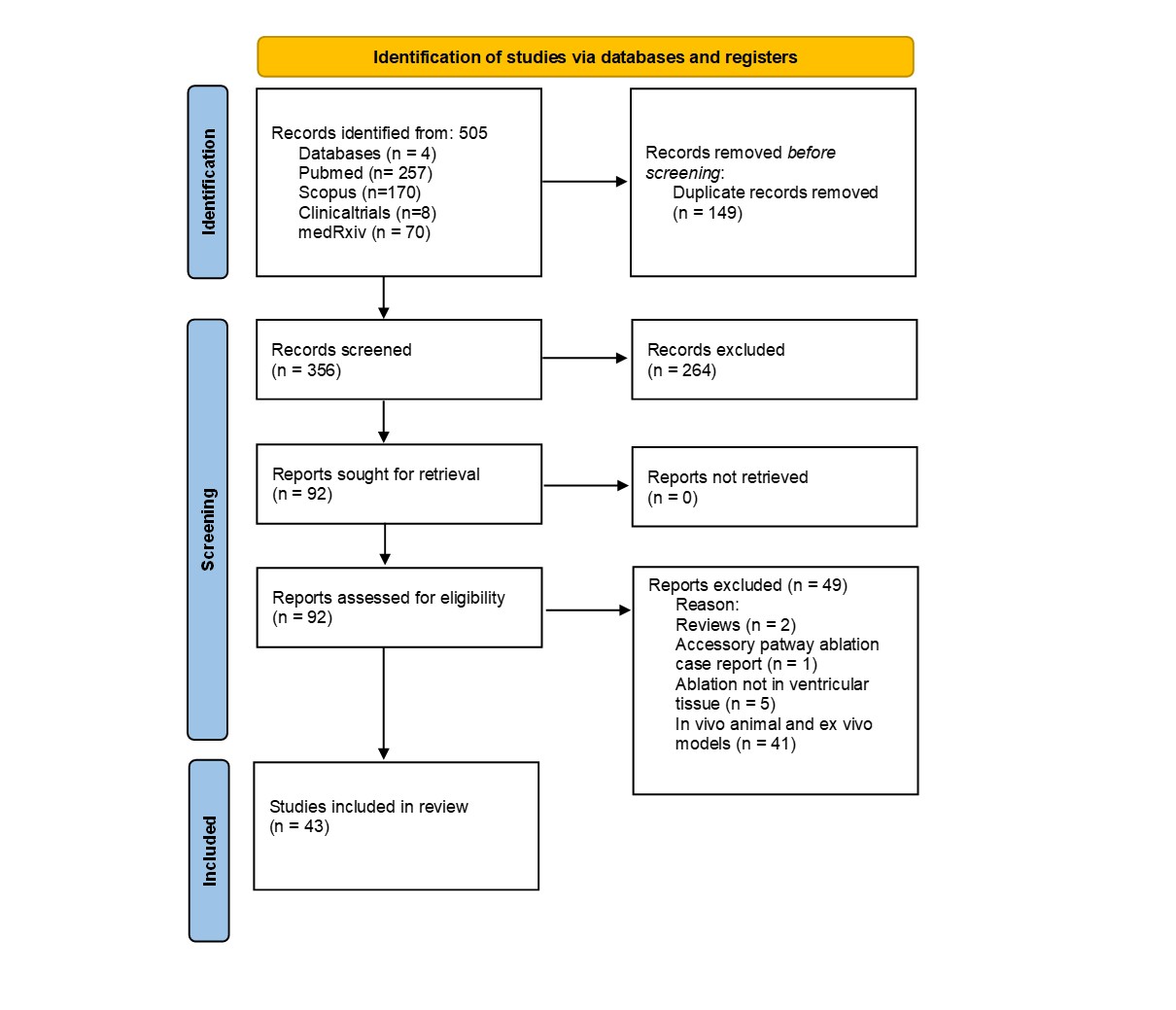
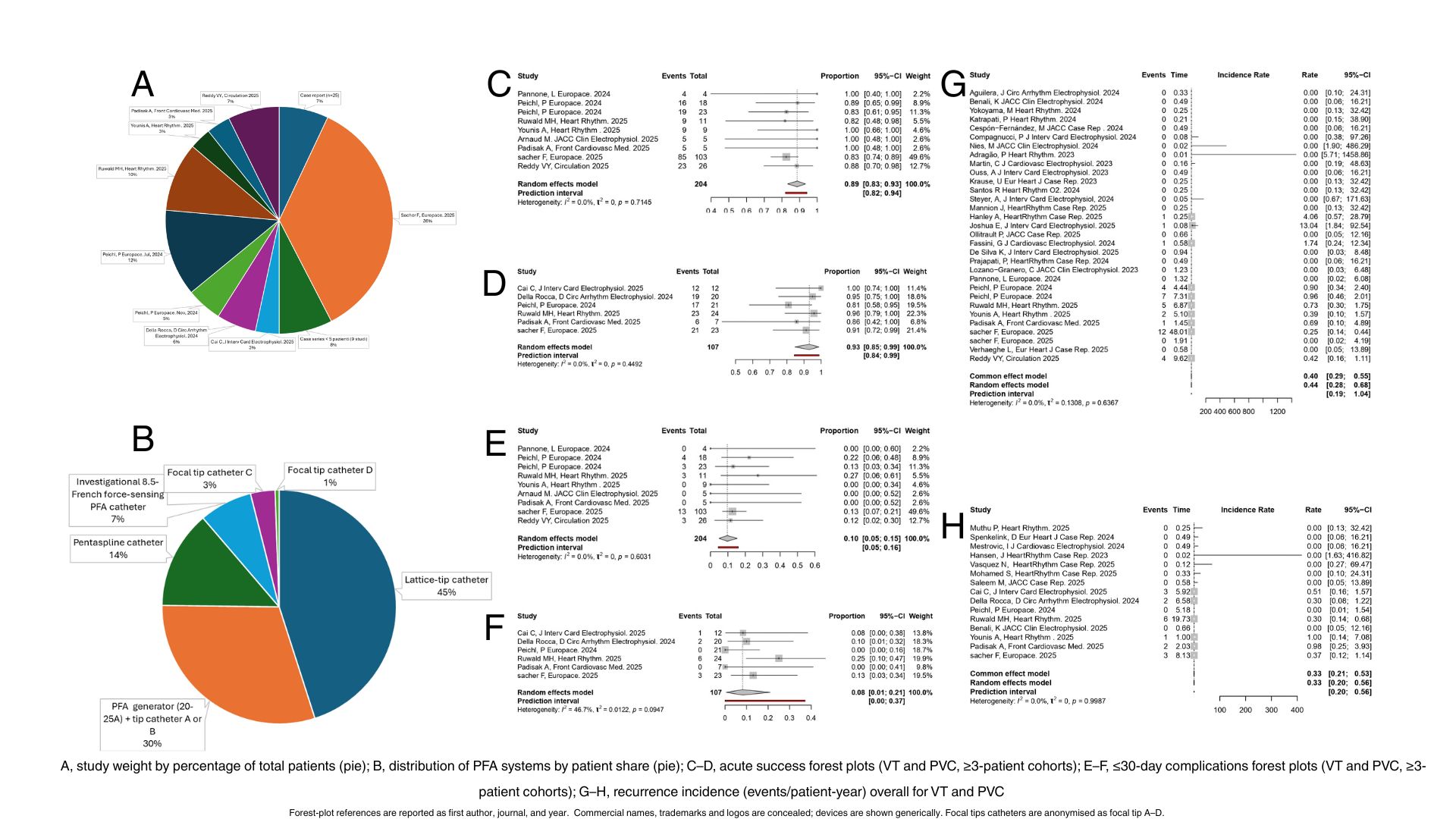
Background: Ventricular pulsed field ablation (PFA) is increasingly adopted for ventricular arrhythmias, yet the evidence base remains fragmented. Purpose: To pool outcomes of ventricular PFA across indications (PVC, VT), estimate between-study heterogeneity, and test robustness in analyses restricted to cohorts with ≥3 patients. Methods: We performed a systematic review and meta-analysis of clinical reports to 10 October 2025. Primary endpoints were: (1) acute success (PVC: elimination of the clinical focus; VT: non-inducibility), (2) intra/≤30-day complications, and (3) recurrence incidence (events per patient-year) at longest follow-up. Proportions were synthesised with generalised linear mixed models. Recurrence was modelled using mixed-effects Poisson models with a person-time offset. Overlapping reports were de-duplicated at patient level; a prespecified sensitivity included only cohorts with ≥3 patients. Results: 355 patients (PVC 122, VT 233) from 43 studies were included; mean age 59.3±14.8 years. Mean LVEF was 53.9±11.7% in PVC and 34.8±12.6% in VT. Redo procedures in 43% of all index PFA sessions. Main etiology was ischemic cardiomyopathy in VT group (51%) and idiopathic in PVC group (72%). Mean follow-up was ~5 months (PVC 155±79 days; VT 152±44 days). Six distinct PFA ablation systems were identified across studies. Hybrid workflows (PFA+RF) occurred in 38%. On average, JBI risk of bias ratings were moderate. (1)Acute effectiveness: In ≥3-patient cohorts, pooled success was 93% (95% CI 85–99; I²=0%) for PVC and 89% (95% CI 83–93; I²=0%) for VT. When all studies were pooled, estimates were ≈100% (PVC) and ≈99% (VT), with I²=0% for both, consistent with small-study/publication effects. (2)Safety (≤30 days): In ≥3-patient cohorts, complications were 8% (95% CI 1–21; I²≈47%) for PVC and 10% (95% CI 5–15; I²=0%) for VT. Across all studies, model-based pooled proportions were ≈1% with I²=0% in both indications (3)Recurrence: Incidence was 0.33 events/patient-year for PVC (I²=0%) and 0.40–0.44 for VT, with modest heterogeneity for VT (I²≈28% in ≥3-patient analyses); the VT prediction interval was ≈0.19–1.25 events/patient-year, reflecting variability in substrate, approach, and surveillance. Conclusion: Across heterogeneous platforms and workflows, ventricular PFA demonstrates high acute effectiveness and near-term safety, and acceptable mid-term durability. Estimates restricted to ≥3 patients studies appear more generalisable than all-study pools.