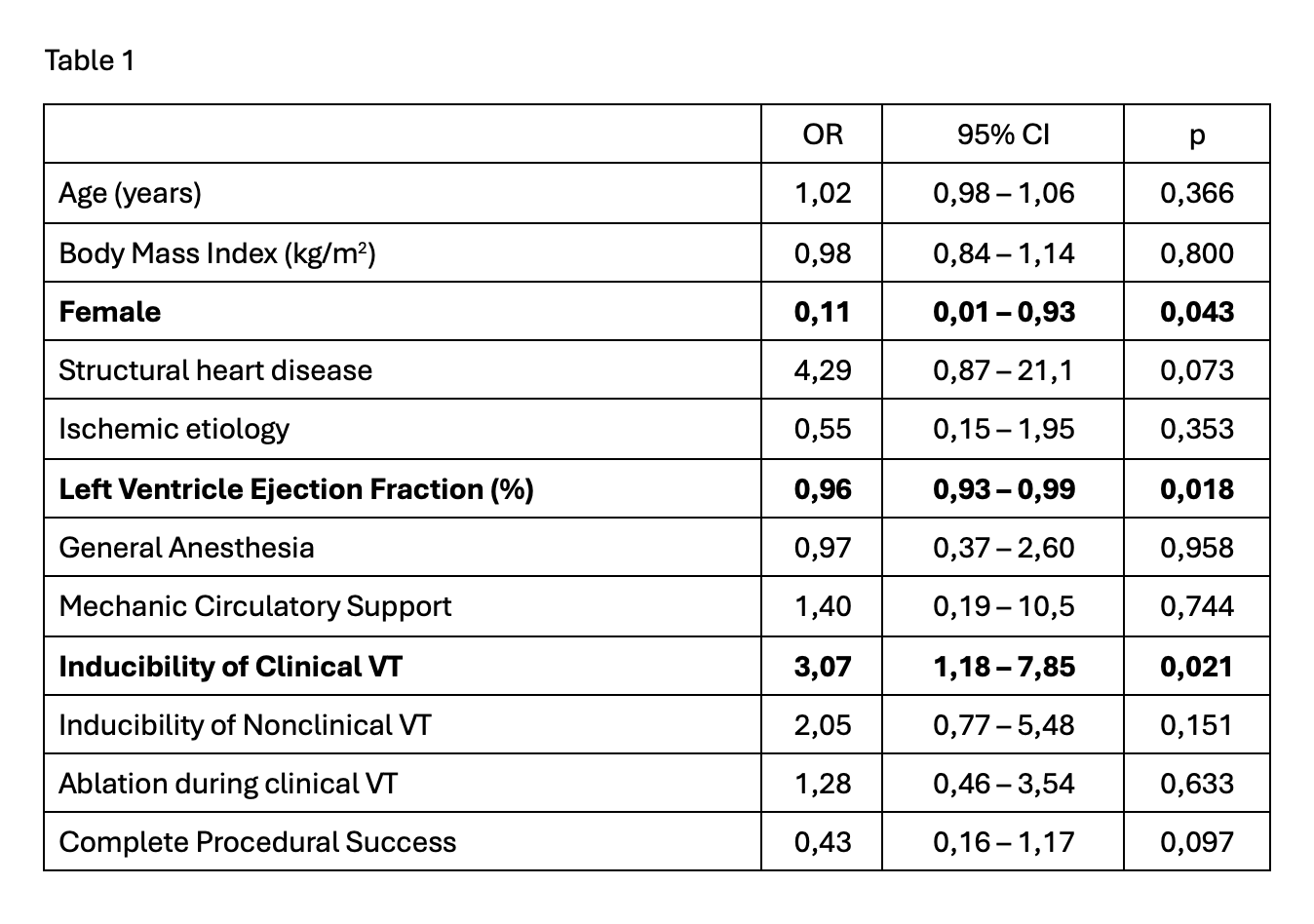
Background Catheter ablation is a key therapeutic strategy for ventricular tachycardia (VT). Nonetheless, a standardized gold-standard procedural strategy has yet to be defined. Methods We retrospectively analysed all consecutive patients treated with VT ablation at our centre between May 2011 and August 2025. The impact of procedural variables on VT recurrence (i.e. documented sustained VT or appropriate ICD therapy) after 24 months from ablation was assessed with logistic regression analyses. Acute procedural success was defined as non-inducibility at Programmed Electrical Stimulation (PES) or abolition of abnormal potentials. Results A total of 105 VT ablation procedures were performed, 90 first procedures and 15 redo ablations. Median age was 69 years (IQR 58 – 74) and 87% were male. Structural heart disease was present in 82% (64% ischemic); median left ventricle ejection fraction (LVEF) was 34% (IQR 25–50%). Clinical VT was induced and mappable in 44 cases (42%), 88 patients (84%) underwent endocardial ablation, and 17 patients also required epicardial access. General anesthesia and mechanical circulatory support were used in 34% and 5% of cases, respectively. Acute procedural success was obtained in 69 patients (66%). Follow-up data (available for 80 patients) showed arrhythmic recurrence in 27 patients (34%) at 12 months and in 32 patients (40%) at 24 months. Female gender (OR 0,11; 95% CI 0,01 – 0,93; p=0,043) and higher LVEF (OR 0,96; 95% CI 0,93 – 0,99; p=0,018) were associated with a reduced risk of recurrence. Among procedural variables (Table 1), pre-ablation clinical VT inducibility significantly increased risk of recurrence (OR 3,07; 95% CI 1,18–7,95; p = 0,021) and acute success showed a protective trend, although not statistically significant ( OR 0,43; 95% CI 0,16–1,17; p = 0,097) . No significant difference in recurrence was found between activation-guided (during VT) vs. substrate-based ablation (p=0.633). Conclusions Our real-world single-centre experience suggests that a procedural strategy targeting clinical VT versus a substrate-based approach does not significantly impact long-term procedural efficacy. While acute success showed a protective trend, pre-procedural inducibility of clinical VT appears to be a marker for increased recurrence risk. Larger studies are warranted to confirm these findings.