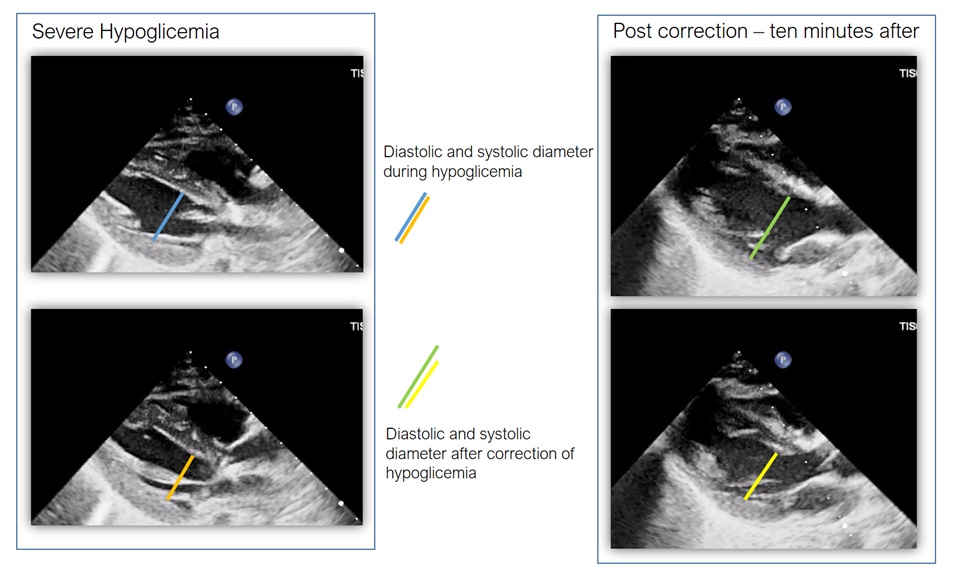
Reversible causes of pulseless electrical activity (PEA) are classically categorized into the “4 H’s and 4 T’s”: H ypovolemia, H ypoxia, H ydrogen ion excess (acidosis), H ypo-/ H yperkalemia , and T ension pneumothorax, Cardiac T amponade, T oxins, T hrombosis . This scheme is usually reported for pediatric and adult population but, while the adult heart relies primarily on fatty acid metabolism, the pediatric myocardium—especially in stress states—shows a much higher dependence on glucose as an immediate energy substrate. This metabolic vulnerability may have relevant clinical implications in conditions of stress and notably, hypoglycemia is not included among pediatric PEA causes despite the recognized metabolic role. We report the case of a child with severe polytrauma complicated by acute hepatic injury. There was no cardiac injury as testified by admission echocardiogram showing normale heart function and structures. During hospitalization, (12 hours later) the patient developed a state of PEA characterized by severe left ventricular disfunction (EF 10%), with no structural abnormalities, no pericardial effusion, no evidence of right ventricular strain, and no signs of mechanical obstruction. Arterial blood gas analysis revealed severe metabolic acidosis and profound hypoglycemia. In the absence of other causes hypoglycemia emerged as the only identifiable acute derangement. Intravenous glucose administration resulted in rapid normalization of blood glucose levels. Remarkably, within approximately 10 minutes, the LVEF improved to 35%, without any significant additional interventions. The abrupt and isolated recovery of systolic performance strongly suggested that severe hypoglycemia played a direct and reversible role in precipitating myocardial depression and a pseudo-PEA state. Given the patient’s hepatic impairment, reduced metabolic reserves likely amplified the myocardial susceptibility to glucose depletion. To our knowledge, this is the first reported pediatric case in which severe hypoglycemia appears to have contributed to the development of pseudo-PEA and profound yet rapidly reversible systolic dysfunction. This case highlights the need to recognize hypoglycemia as a potential contributor to cardiovascular collapse in metabolically vulnerable children. We propose that, in pediatric advanced life support, hypoglycemia should be considered as an additional reversible cause alongside the traditional 4 H’s and 4 T’s.