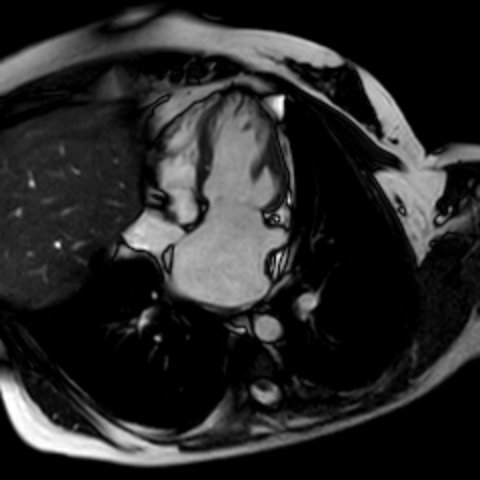
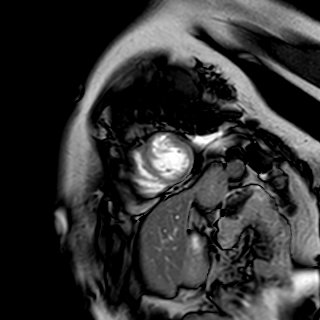
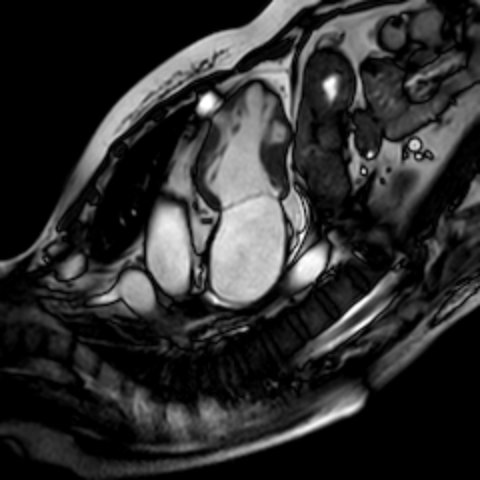
Saw-tooth cardiomyopathy (STC) is a rare form of left ventricular cardiomyopathy , characterised by an irregular, “saw-tooth” endocardial contour with myocardial projections extending from the lateral walls towards the ventricular cavity. This pattern is distinct from LVNC. It is a newly discovered cardiomyopathy, first described in 2009, and to date it is not recognised as a distinct nosological entity in current cardiomyopathy classifications. Its clinical significance and prognostic implications remain incompletely defined. Available evidence, mainly derived from case reports and small series, suggests an association with heterogeneous clinical manifestations (1, 2). The potential relationship between this morphological pattern and the development of heart failure with preserved ejection fraction (HFpEF) has been poorly explored. We present the case of a 36-year-old with an unremarkable past medical history. No family history of cardiovascular disease or sudden death. She was admitted to for atrial fibrillation associated with clinical manifestation of heart failure. Laboratory tests were unremarkable, except for NT-proBNP level (1196 pg/mL). The echocardiogram showed a trabeculated appearance of the interventricular septum and inferior wall, with a normal ejection fraction (68%) and increased left ventricular filling pressures. Cardiac magnetic resonance showed a multiple protrusions of the compacted myocardial layer into the ventricular cavity, consistent with a possible “saw-tooth” cardiomyopathy, in the absence of inflammatory myo-pericardial alterations. Following clinical stabilisation, transcatheter ablation of atrial fibrillation was successfully performed. In the absence of specific evidence from the literature, HFpEF-directed therapy with empagliflozin was initiated. At both six-month and one-year follow-up, the patient remained haemodynamically stable. NT-proBNP levels showed a reduction but remained persistently elevated (medium value 960 pg/mL). In this case STC may be considered the underlying cause of HFpEF. Advanced cardiac imaging plays a key role in the diagnostic work-up, while management requires an individualised, phenotype-driven approach. Further studies are needed to clarify the clinical significance, optimal management, and prognostic implications of this cardiomyopathy. Chenaglou M et al. ESC Heart Failure 2020; 7: 325–328 DOI: 10.1002/ehf2.12574 Liu Z et al. Rev. Cardiovasc. Med. 2022; 23(4): 138 doi.org/10.31083/j.rcm2304138