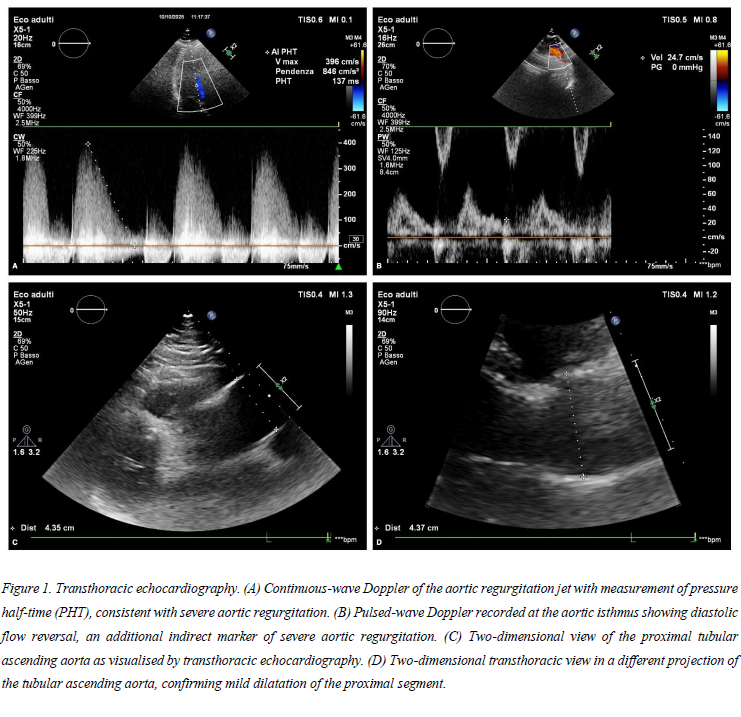
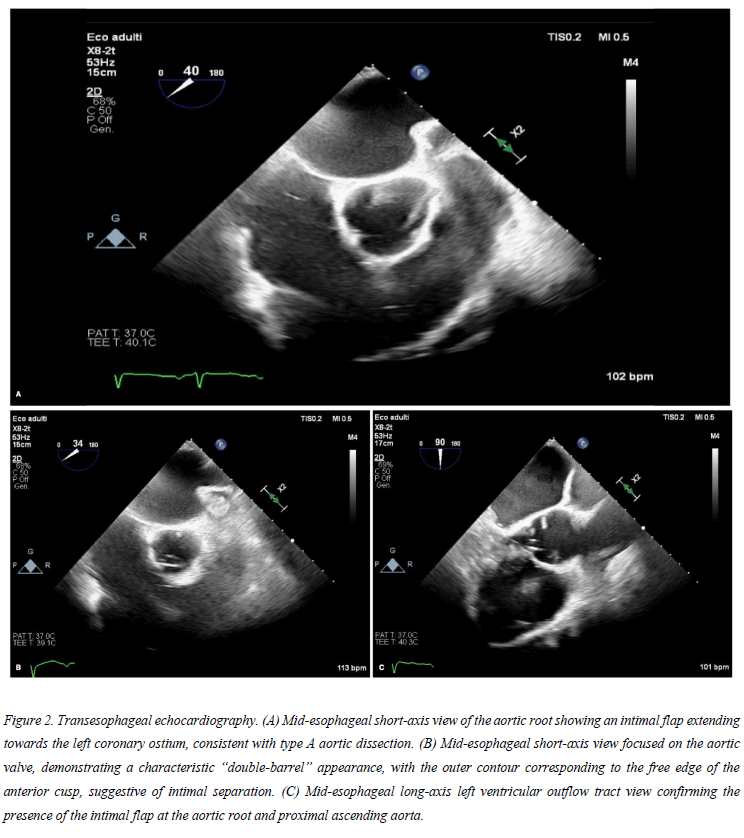
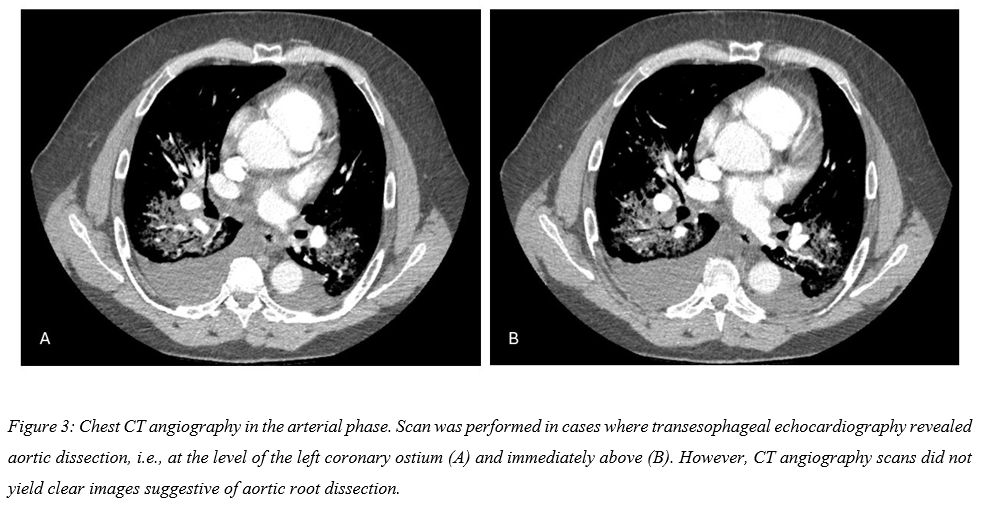
Background: Type A aortic dissection is a life-threatening emergency. Painless forms, especially when computed tomography angiography (CTA) is non–ECG-gated and performed for non-aortic indications, may escape diagnosis. Transesophageal echocardiography (TEE) can be crucial when acute severe aortic regurgitation and heart failure are present, particularly if the clinical picture is not typical. Case presentation: A 52-year-old hypertensive, obese man with a history of intravenous and inhaled drug abuse presented to a peripheral emergency department with acute dyspnoea and pulmonary oedema, without chest pain. D-dimer levels were elevated and a thoracic CTA, performed to rule out pulmonary embolism, was negative for embolism and showed no clear aortic abnormalities. Transthoracic echocardiography (TTE) revealed severe eccentric aortic regurgitation with only mild dilatation of the ascending aorta and no signs of left ventricle chronic volume overload, leading to transfer to a tertiary cardiology center. TEE demonstrated an intimal flap at the aortic root extending towards the left coronary ostium, consistent with Stanford type A dissection. A second urgent aortic CTA again failed to show definite signs of dissection. Given the high clinical suspicion and the strongly suggestive TEE findings, the multidisciplinary heart team, including cardiologists, cardiac surgeons and imaging specialists, decided to proceed with emergency surgery. Intraoperative inspection confirmed an acute type A aortic dissection with a circumferential intimal tear along the sinotubular junction, extending to the aortic annulus, and a false lumen confined to the aortic root and proximal ascending aorta; both coronary ostia were anatomically intact. The patient underwent a Bentall procedure with replacement using a 28-mm Dacron valved conduit with a 25-mm pericardial bioprosthesis and coronary button reimplantation, together with left atrial appendage closure, with an uneventful postoperative course. Conclusions: This case illustrates an atypical painless presentation of type A aortic dissection, dominated by acute heart failure due to severe aortic regurgitation in the absence of chest pain. It highlights the limitations of non–ECG-gated CTA performed for non-aortic indications and underscores the pivotal role of TEE in establishing the diagnosis and guiding life-saving management when clinical probability remains high despite a negative CTA.