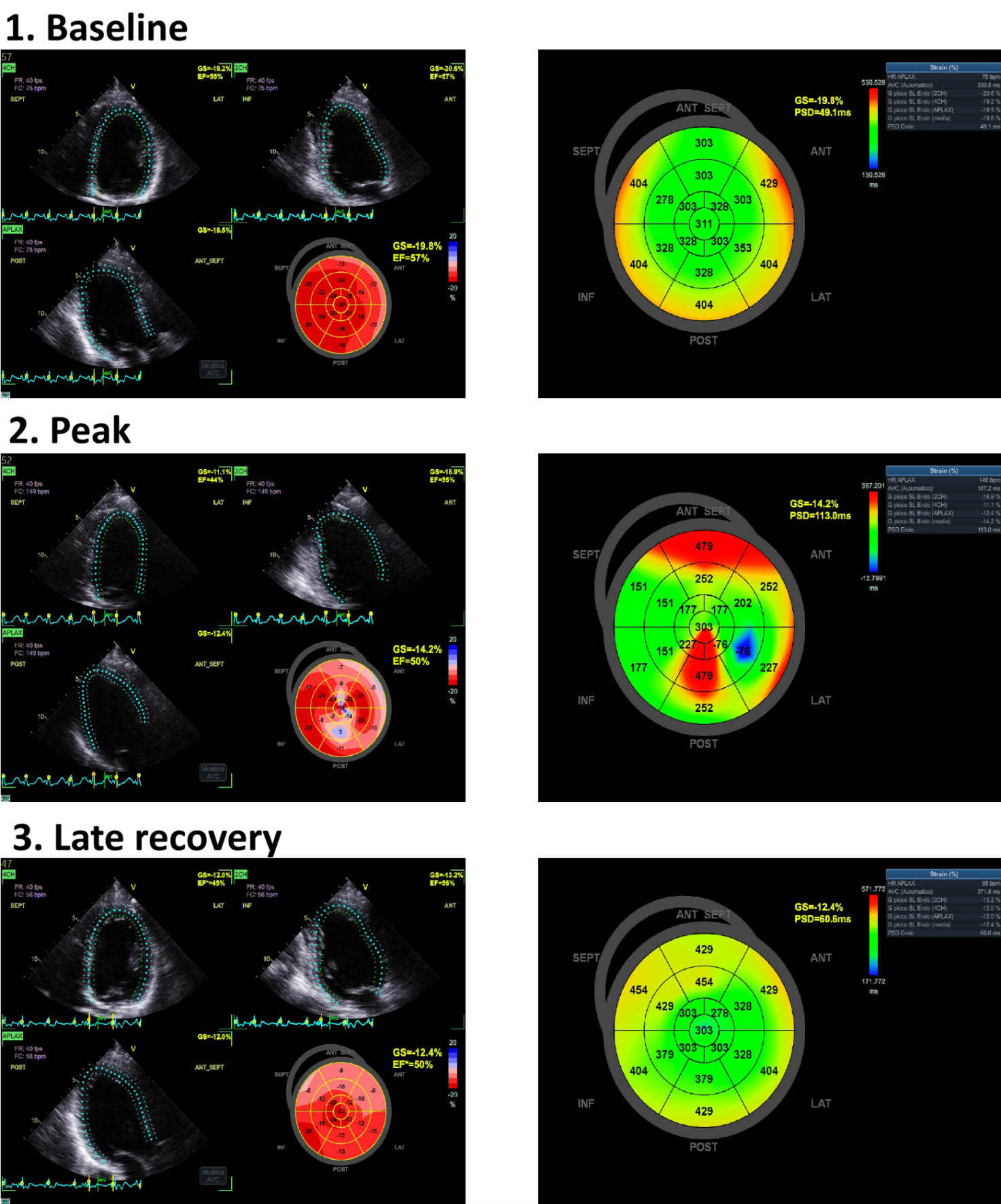
INTRODUCTION Myocardial bridges are common congenital coronary anomalies in which a segment of an epicardial artery—most often the left anterior descending (LAD)—takes an intramyocardial course. Systolic compression and delayed diastolic expansion of the tunneled segment may produce dynamic flow limitation, potentially leading to ischemia‑related ST–T changes or arrhythmias. Speckle tracking echocardiography (STE) provides angle‑independent assessment of myocardial deformation and can detect subtle systolic dysfunction through parameters such as global longitudinal strain (GLS). AIM The aim is to evaluate whether STE during stress echocardiography may help raise suspicion of myocardial bridging in athletes by identifying regional strain abnormalities. MATERIALS AND METHODS Ten male athletes (aged 37–65 years) underwent stress echocardiography testing on a on a bicycle ergometer (COSMED), in a semi-supine position. Imaging was performed with a GE HealthCare Vivid S70 system, and STE analysis was conducted using EchoPAC. Exercise protocols were individualized (maximum workload 320 W; mean 240 W), and all subjects reached criteria for maximal testing. Images were analyzed at baseline, peak exercise, and late recovery for GLS, post‑systolic delay (PSD), and peak systolic index (PSI). RESULTS No wall‑motion abnormalities were observed, and ejection fraction was preserved in all subjects. Two athletes showed isolated ventricular ectopic beats and borderline ST–T changes without diagnostic significance. Mean GLS values were borderline relative to reference norms (baseline −17%; peak −15%; late recovery −19%). All patients demonstrated regional strain abnormalities—including PSD and PSI changes—localized to the myocardial territory supplied by the suspected bridged artery. DISCUSSION Despite normal wall‑motion assessment and absence of clear ischemic ECG changes, STE revealed borderline GLS values and consistent regional strain alterations corresponding to the territory of the tunneled artery (Figure). These findings suggest that STE may provide additional functional insight in athletes with suspected myocardial bridging. Larger studies are needed to determine whether strain‑based analysis can enhance early identification and risk stratification of myocardial bridges.