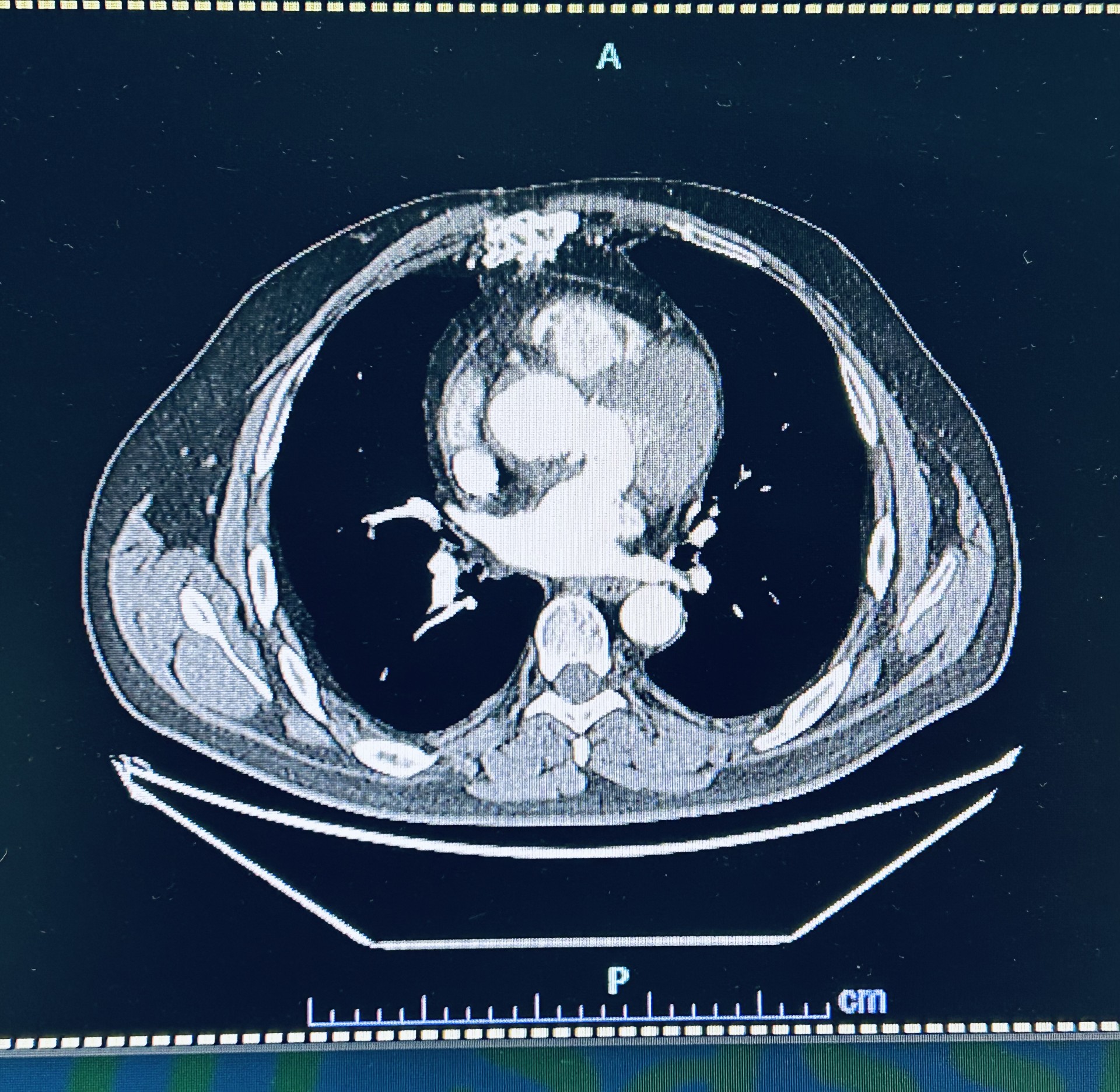
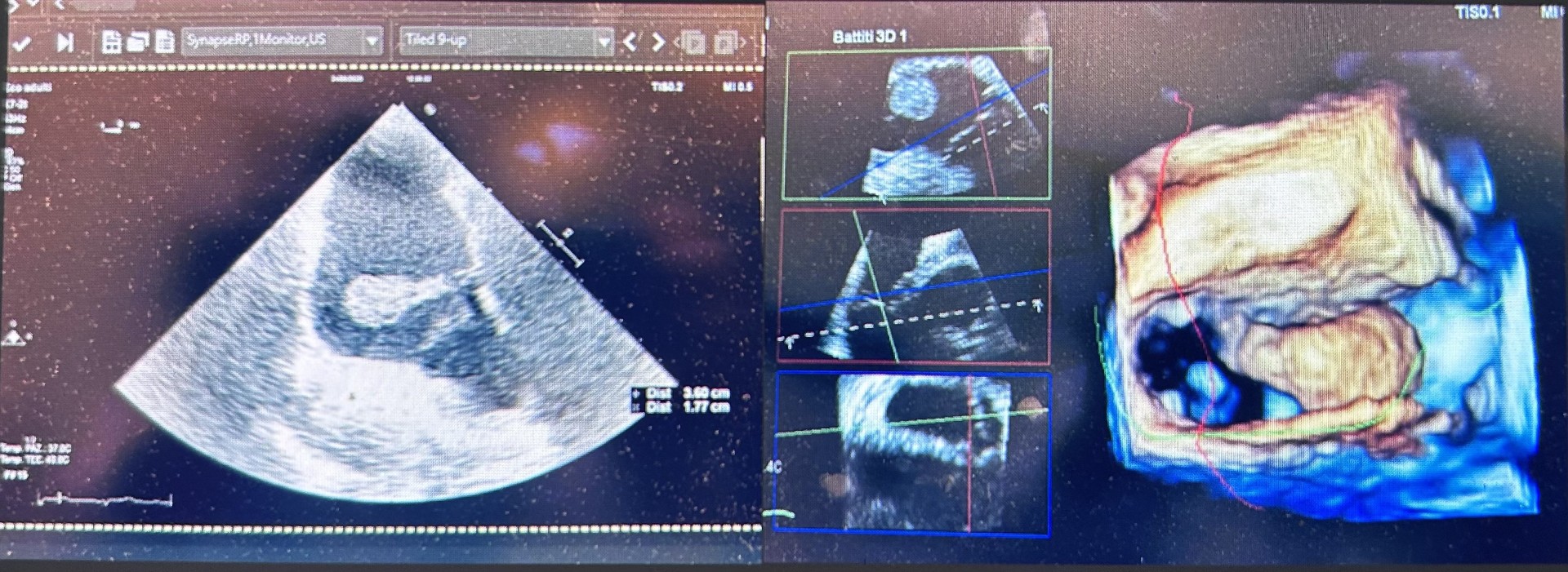
Extracorporeal circulation is associated with a hypercoagulable state that cannot always be controlled with heparin. We present the case of a patient with a massive right atrial thrombosis diagnosed approximately 6 months after ascending aortic valve replacement surgery with native aortic valve resuspension (Tirone David). Case Report A 60-year-old man, 190 cm tall and weighing 102 kg, with dyslipidemia, arrived in the emergency room after a postoperative chest CT scan showing a right atrial mass described as a "filling defect" and a periaortic rim approximately 4 cm long (Fig. 1). His medical history included thyroidectomy for multinodular goiter and COPD with CPAP. Six months earlier, he had undergone valve-sparing surgery without complications. The ECG and laboratory tests were normal, particularly the complete blood count and inflammatory markers. A fast echocardiogram (TTE) showed a right atrial mass floating in the ventricle, measuring approximately 3.5 x 2 cm, with an enlarged ascending aorta, normal left ventricular systolic function, and non-dilated atria. Elective TTE and transesophageal echocardiogram (TEE) revealed that the pedunculated mass was anchored to the atrial wall adjacent to the insertion of the tricuspid valve septal leaflet (Fig. 2). The patient was asymptomatic and feverless, making an endocarditic etiology unlikely, although not entirely excluded. After a cardiac surgery consultation (CCH), it was decided to proceed with the mass removal (Fig. 3) with histological confirmation of its thrombotic nature. Normal surgical outcomes were observed in the ascending aorta and the patient had a good clinical recovery. The literature reports cases of deep vein thrombosis after CCH with possible pulmonary embolism, and rare cases of left atrial thrombosis in patients with AF and dilated atria. A possible cause, heparin-induced thrombocytopenia (HIT), present in 1.9% of cardiac surgery patients, was ruled out due to a consistently normal platelet count. This case highlights how intracardiac thrombosis can develop even in the absence of obvious risk factors or symptoms. The atrial location, not directly related to the aortic surgery but still close to the surgical site, raises questions about the origin of the thrombus. The late diagnosis and atypical location underscore the importance of more patient-tailored preventive strategies and possible extension of anticoagulant therapy in patients undergoing complex procedures or at increased risk.