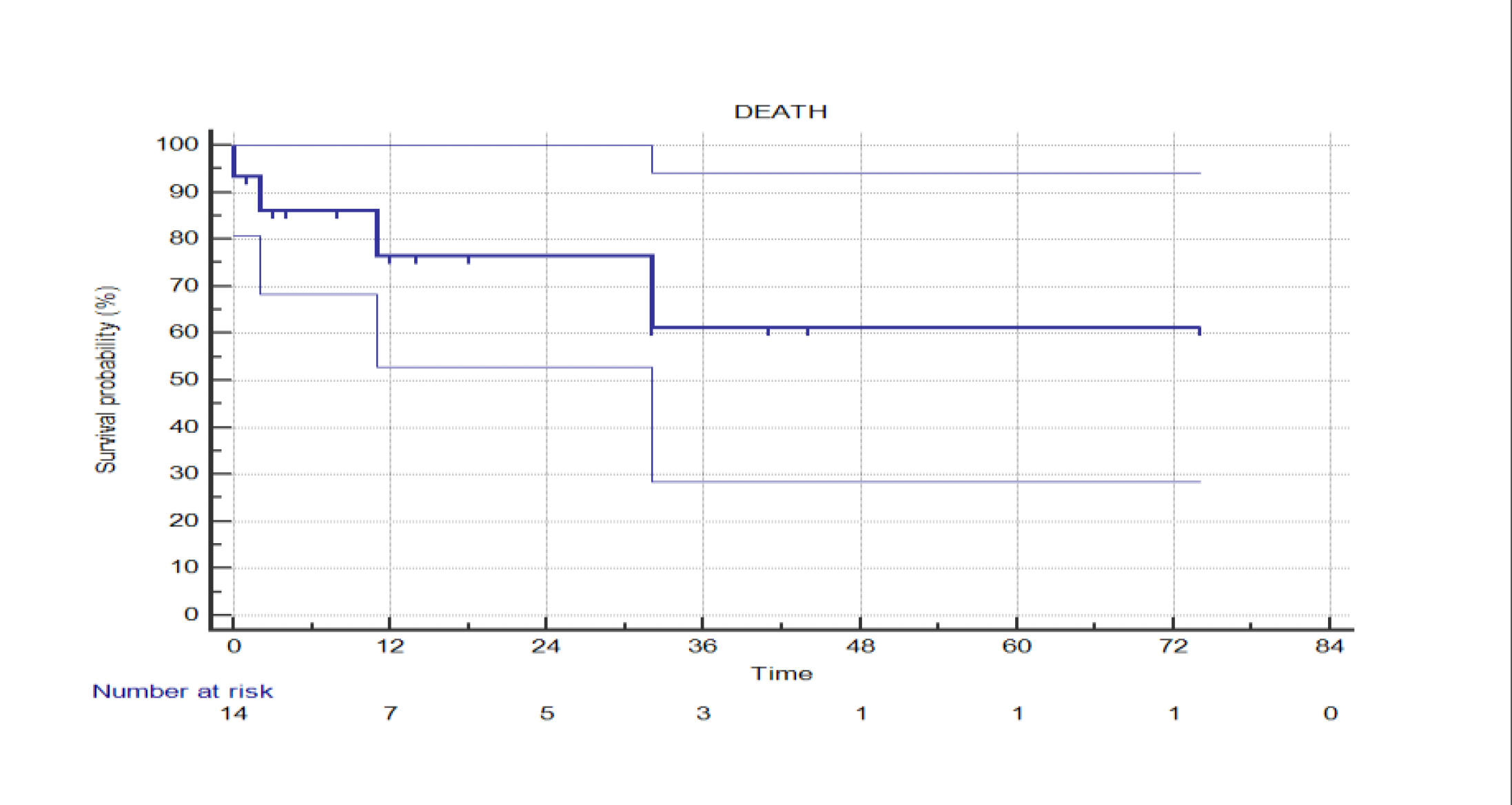
Background and Aim: Transfemoral aortic valve replacement (TAVR) for pure aortic regurgitation (AR) remains under-investigated, with limited data available regarding long-term outcomes. Methods: From January 2019 to June 2025, 15 patients (median age 71 years; range 47–86; 50% female) undergoing TAVR for pure AR were included in this retrospective study. All commercially available TAVR devices were considered. The primary endpoints were in-hospital and late-term mortality. Results : Patients treated with TAVR for AR accounted for 1.5% of the overall TAVR volume. Contraindications to conventional surgery included advanced heart failure (33%), porcelain aorta (6%), complex redo surgeries (13%), and multiple comorbidities in the remaining patients. A balloon-expandable transcatheter heart valve (THV) was implanted in 86% of cases. The 30-day mortality rate was 6%. One patient (6%) experienced acute valve embolization requiring surgical intervention, and another required a second THV due to valve migration Postoperative pacemaker implantation in 20%. Median follow-up was 12 months (range 2–78). Three patients died during follow-up (1 cardiac cause, 1 cancer, 1 liver disease). Freedom from cardiac death at follow-up was 83% ± 11% (table 1). No cases of late THV dysfunction or redo procedures were reported (at follow-up mean transvalvular gradient 9 ± 3 mmHg; LVEF 50% ± 9%). One patient was successfully bridged to heart transplantation as intended, after three years. Conclusions: TAVR for pure AR in selected high-risk patients demonstrated acceptable early and late mortality rates. Despite a non-negligible perioperative complication rate, THV performance at follow-up was favorable, with no cases of recurrent AR, PVL, or valve dysfunction.