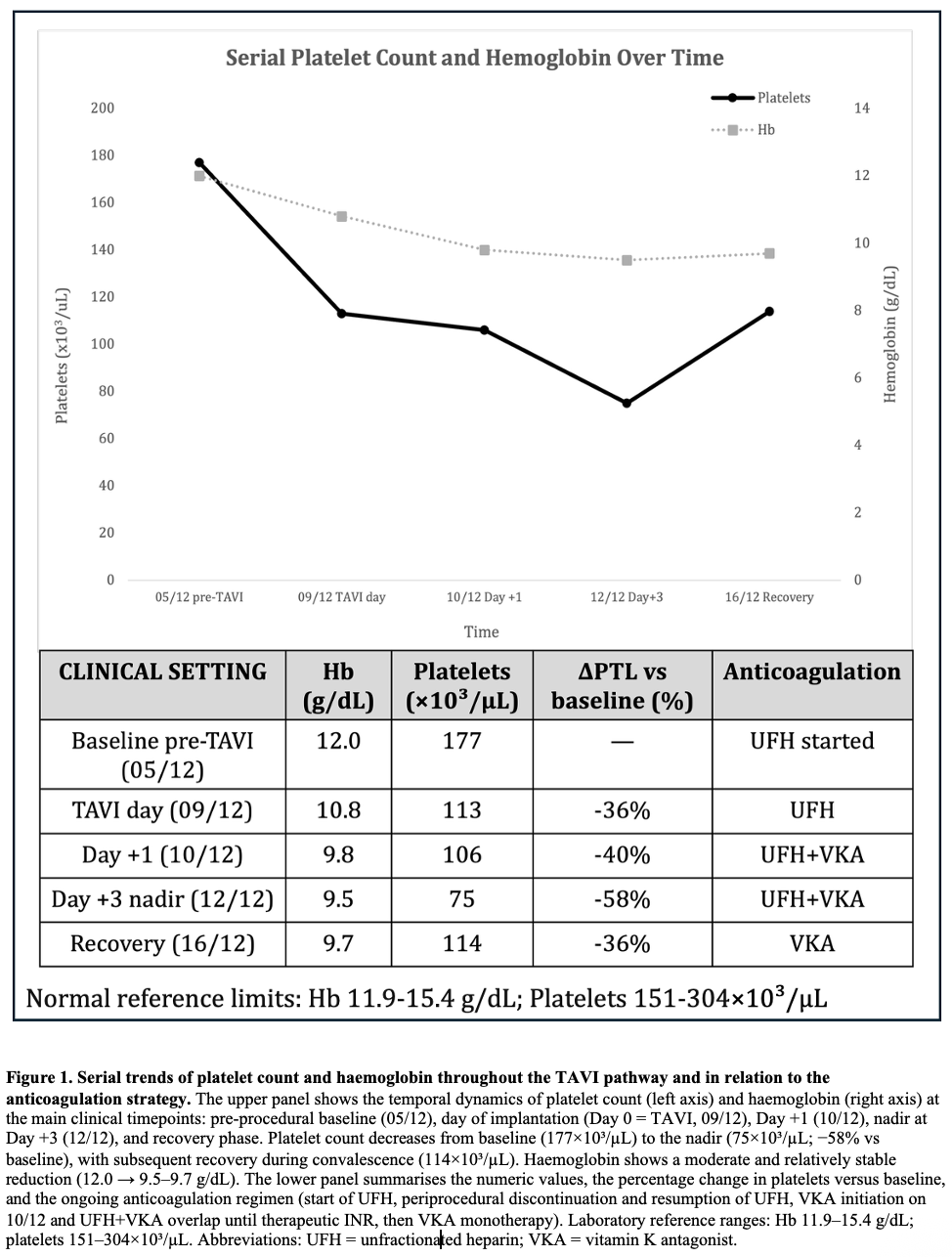
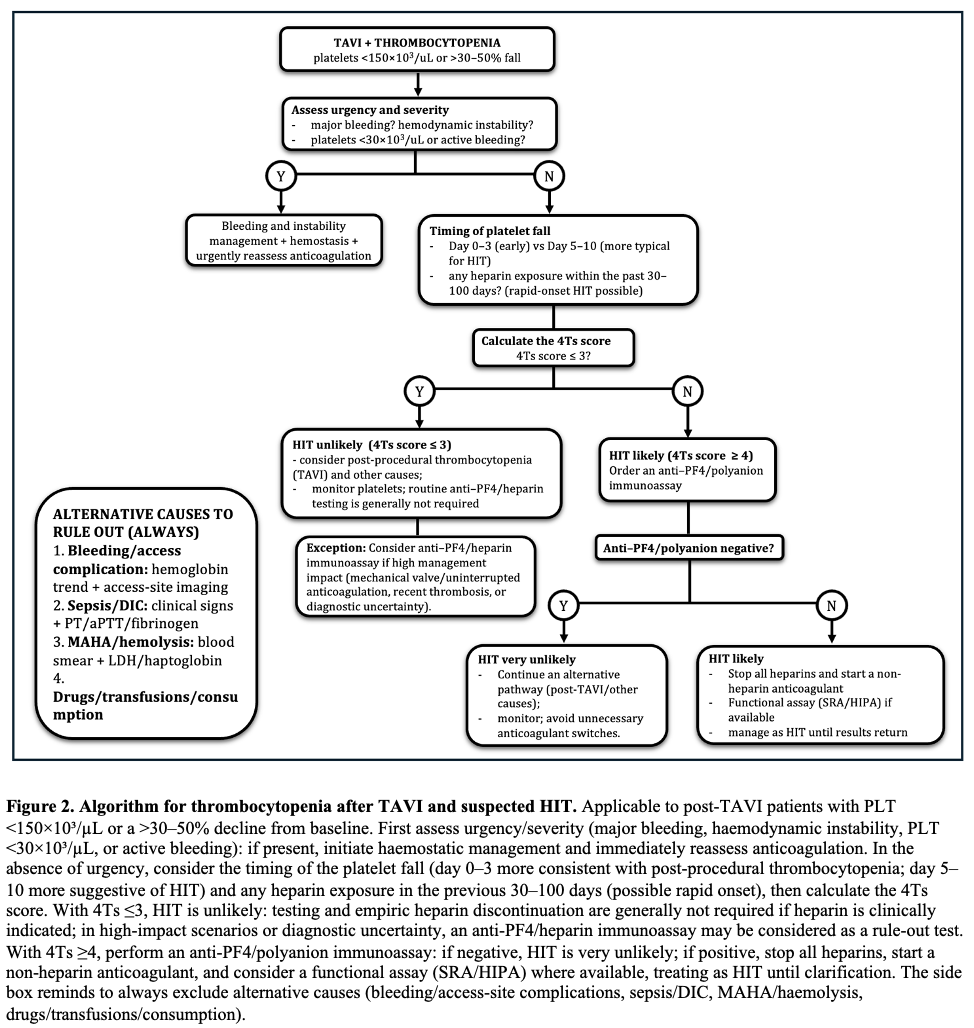
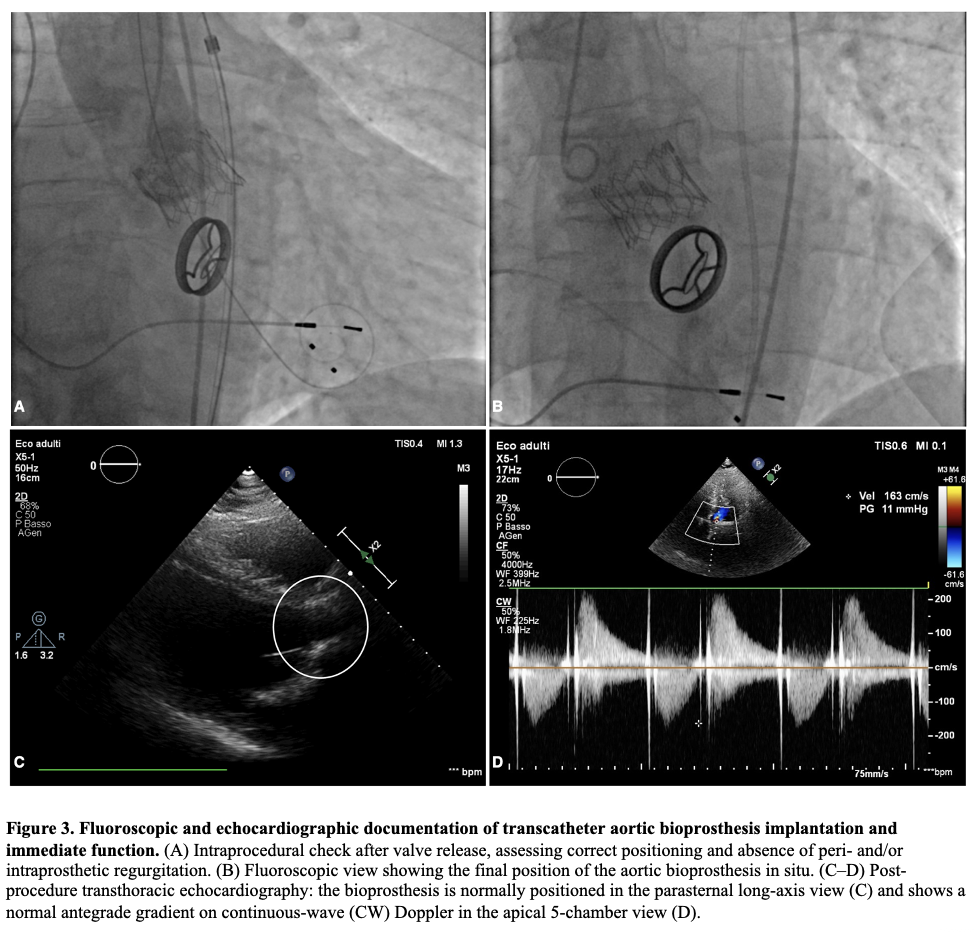
BACKGROUND: Thrombocytopenia is common after transcatheter aortic valve implantation (TAVI) and is often a self-limited procedural phenomenon. In patients requiring peri-procedural heparin bridging, the early platelet drop may raise concern for heparin-induced thrombocytopenia (HIT) and prompt potentially hazardous changes in anticoagulation. CASE PRESENTATION: A 73-year-old man with permanent atrial fibrillation and a mechanical mitral valve on vitamin K antagonist (VKA) underwent transfemoral TAVI for symptomatic severe paradoxical low-flow/low-gradient aortic stenosis. Unfractionated heparin (UFH) bridging was started 4 days before TAVI. The procedure was uncomplicated. Platelets declined from 177×10^3/µL (pre-TAVI) to 113×10^3/µL on day 0, 106×10^3/µL on day +1, with a nadir of 75×10^3/µL on day +3 (−58%), then recovered to 114×10^3/µL by day +7. Haemoglobin decreased from 12.0 to 9.5 g/dL without overt bleeding; vascular access ultrasound excluded haematoma, pseudoaneurysm and arteriovenous fistula. Fibrinogen remained within the normal range (about 230–400 mg/dL). Clinical probability for immune HIT was low (4Ts ≤3) and an anti-PF4/polyanion immunoassay was negative. Given the very high thrombotic risk, UFH was continued as bridging while VKA was restarted, then UFH was stopped after reaching the therapeutic INR. Post-procedural echocardiography confirmed a normally functioning transcatheter valve without significant leak. CONCLUSIONS: An early, marked platelet fall after TAVI—especially with day 0–3 nadir and rapid recovery—may represent a procedural “pseudo-HIT” pattern rather than immune HIT. Integrating timing, pre-test probability and anti-PF4 testing can avoid unnecessary heparin discontinuation or unsafe anticoagulation interruptions in patients with mechanical valves.