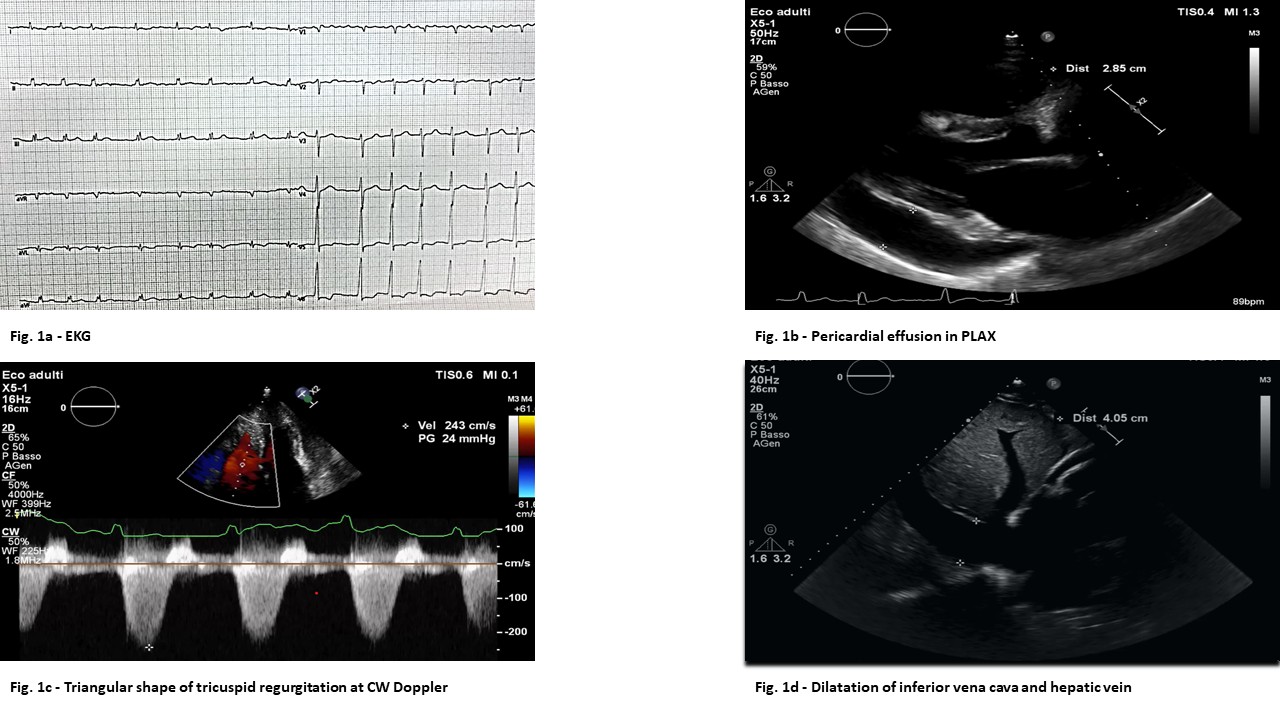
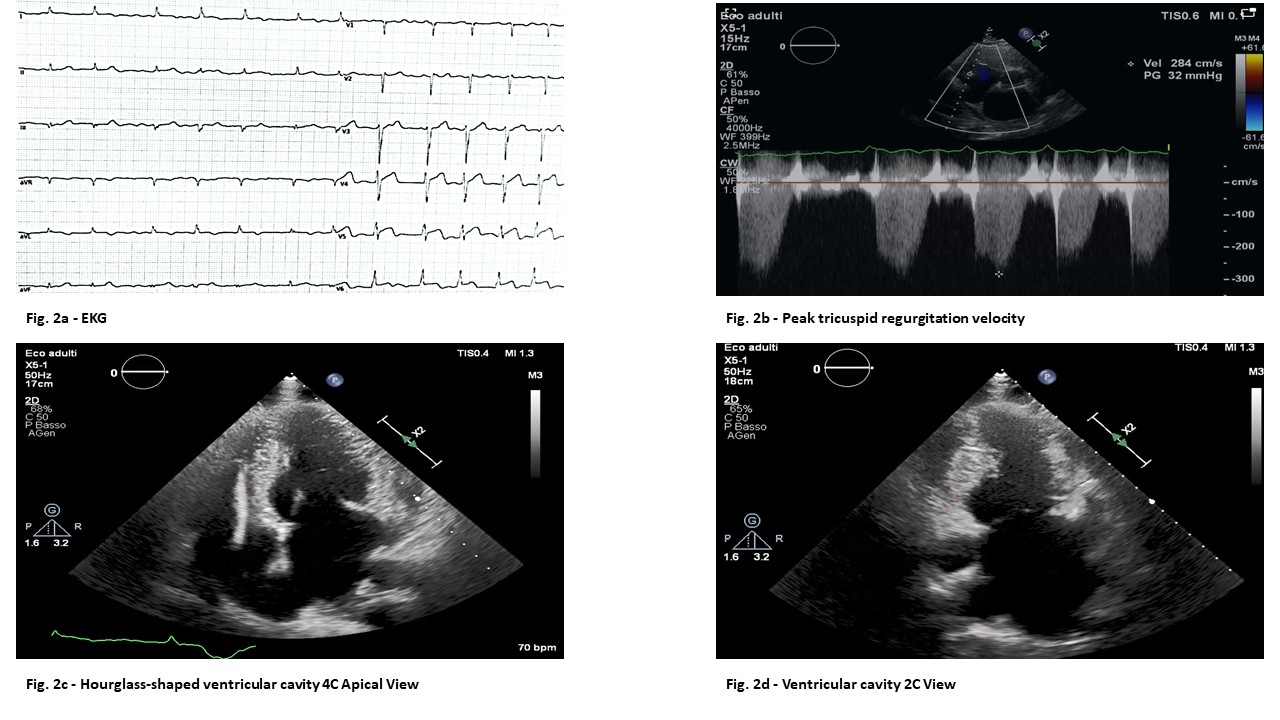
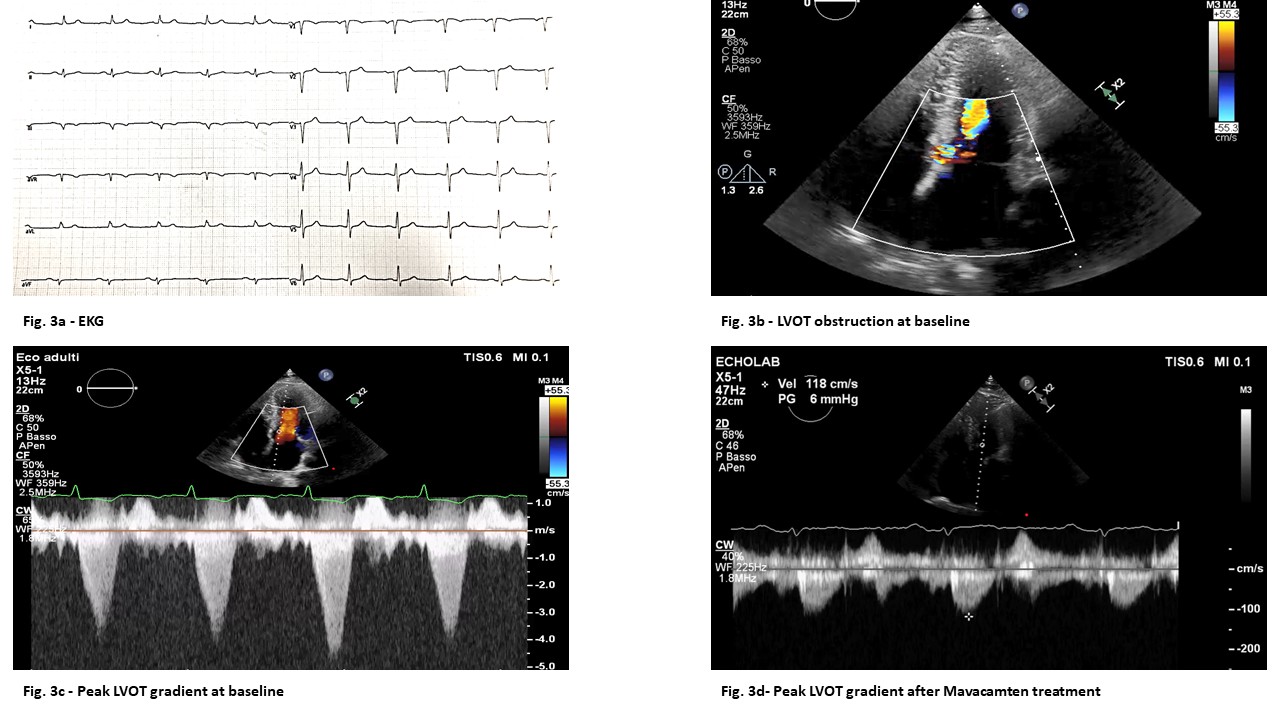
Background: We report a family affected by hypertrophic cardiomyopathy (HCM) caused by a pathogenic variant (c.3192dup p.Lys1065GlnfsTer12) in the MYBPC3 gene, illustrating remarkable phenotypic heterogeneity and a malignant clinical course. Case Presentation: The proband (second-born) was diagnosed at age 17 with obstructive HCM. His clinical course was characterized by progression toward a restrictive phenotype, atrial fibrillation, and severe heart failure. Echocardiography (Fig.1) showed a small, obliterated left ventricular cavity, biatrial dilatation, moderate to severe mitral and tricuspid regurgitation, secondary pulmonary hypertension and severe pericardial effusion. Due to refractory heart failure (NYHA class IV), he underwent cardiac transplantation at age 43. The mother was diagnosed at age 58 during family screening. She presented with asymmetric mid-ventricular hypertrophy and mid-ventricular obstruction, leading to apical aneurysm development during follow-up ( Fig. 2 ), confirmed by MRI which showed apical akinesia with transmural late gadolinium enhancement . Following a progressive decline in functional capacity in NYHA class III-IV, she was recently transplanted. The first-born son was diagnosed at age 36 with classic obstructive HCM ( Fig. 3 ) with LVOT obstruction due to systolic anterior motion of the mitral valve. Given the persistence of significant gradients and symptoms despite beta-blocker therapy, he started compassionate treatment with Mavacamten in 2024. Up-titration to 10 mg led to the complete resolution of the LVOT gradient and a significant improvement in functional class and cardiac biomarkers. All three family members were classified as high risk for sudden cardiac death (SCD) and received an ICD for primary prevention. To date, and until the time of transplantation for the first two cases, no appropriate shocks or ventricular arrhythmias have been recorded. Conclusions: This case highlights how the same MYBPC3 mutation can manifest with extreme phenotypic diversity within a single family—ranging from restrictive evolution, mid-ventricular obstruction with apical aneurysm to classic LVOT obstruction. The clinical course of this family proved to be malignant, requiring cardiac transplantation in two out of three family members.