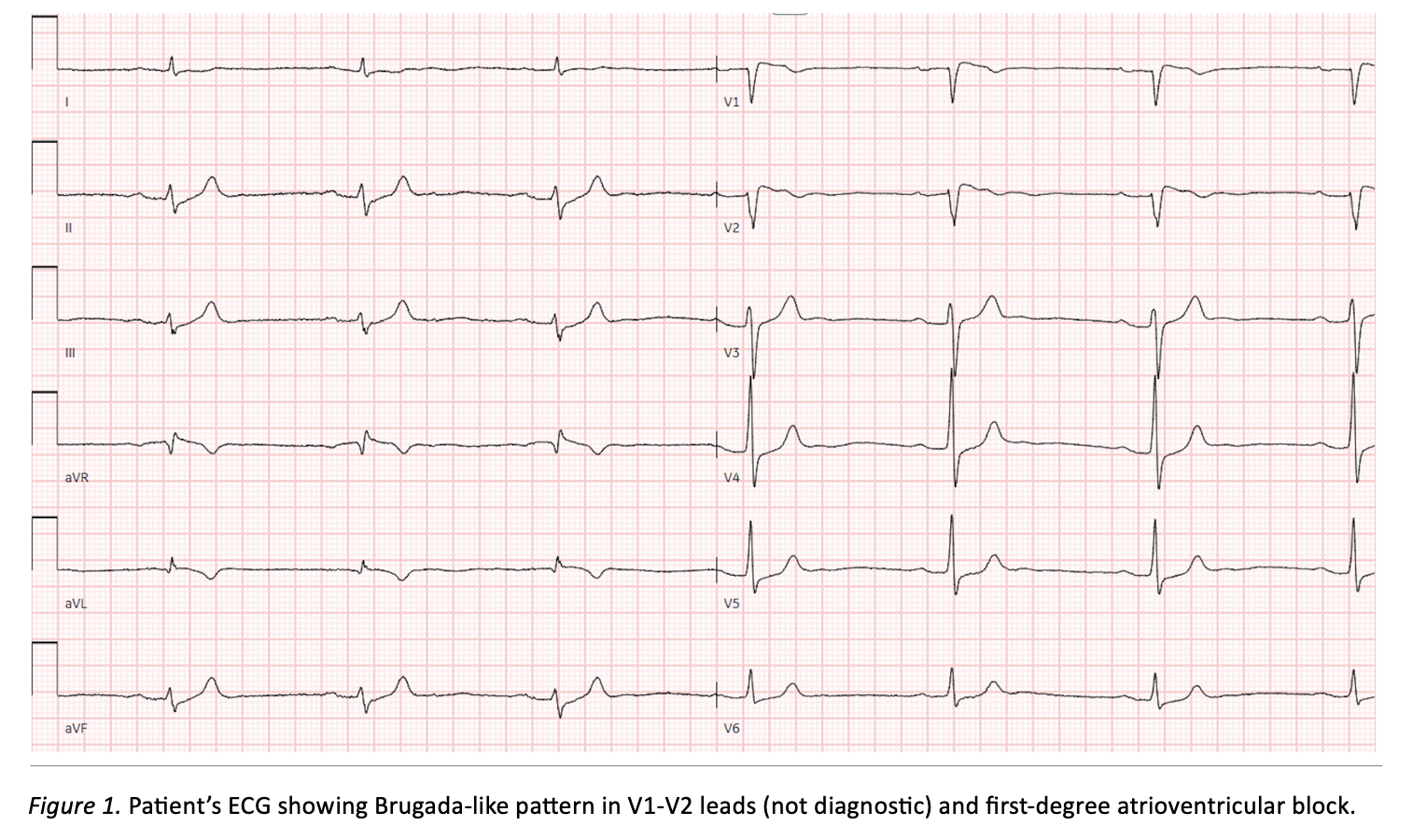
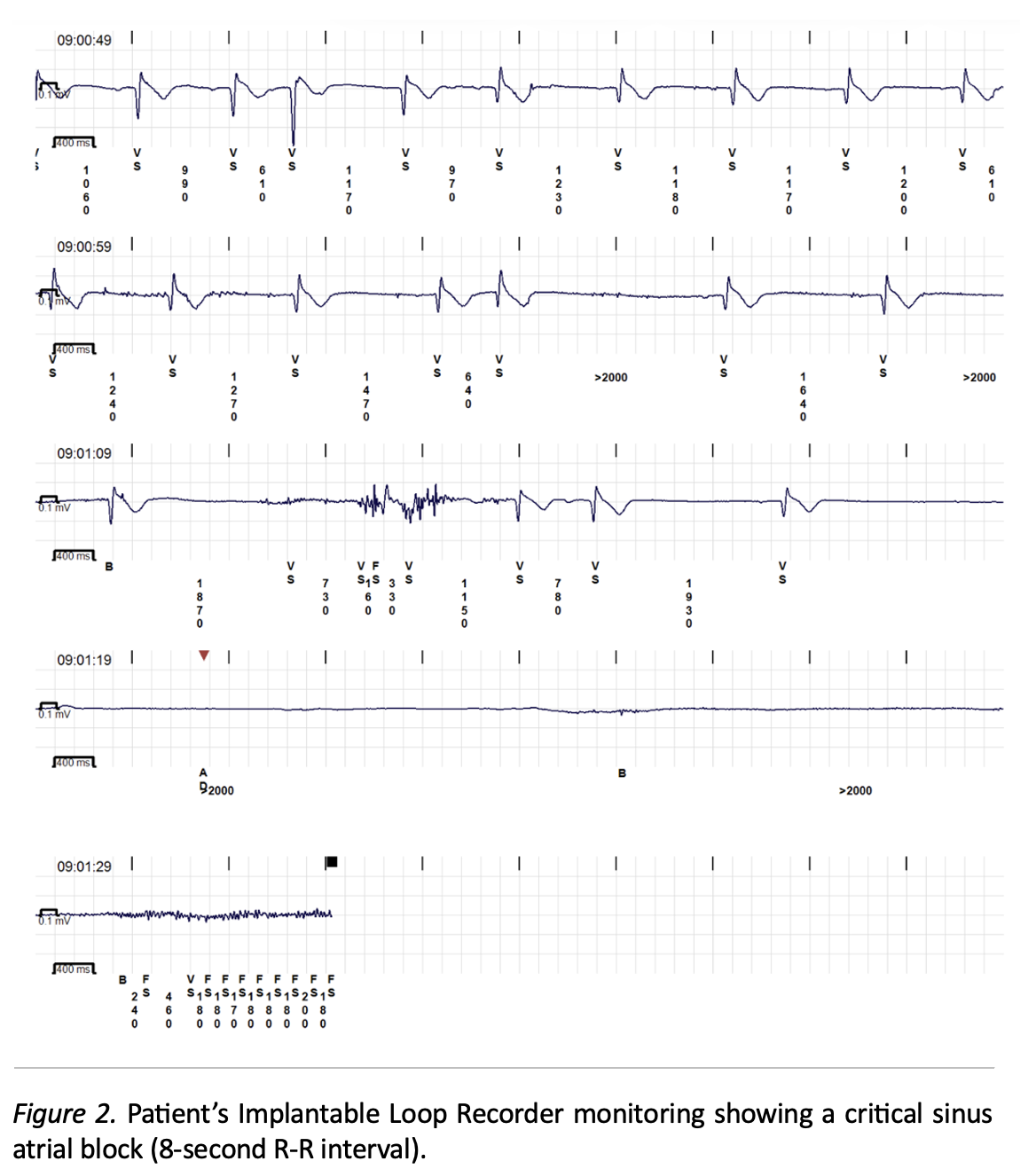
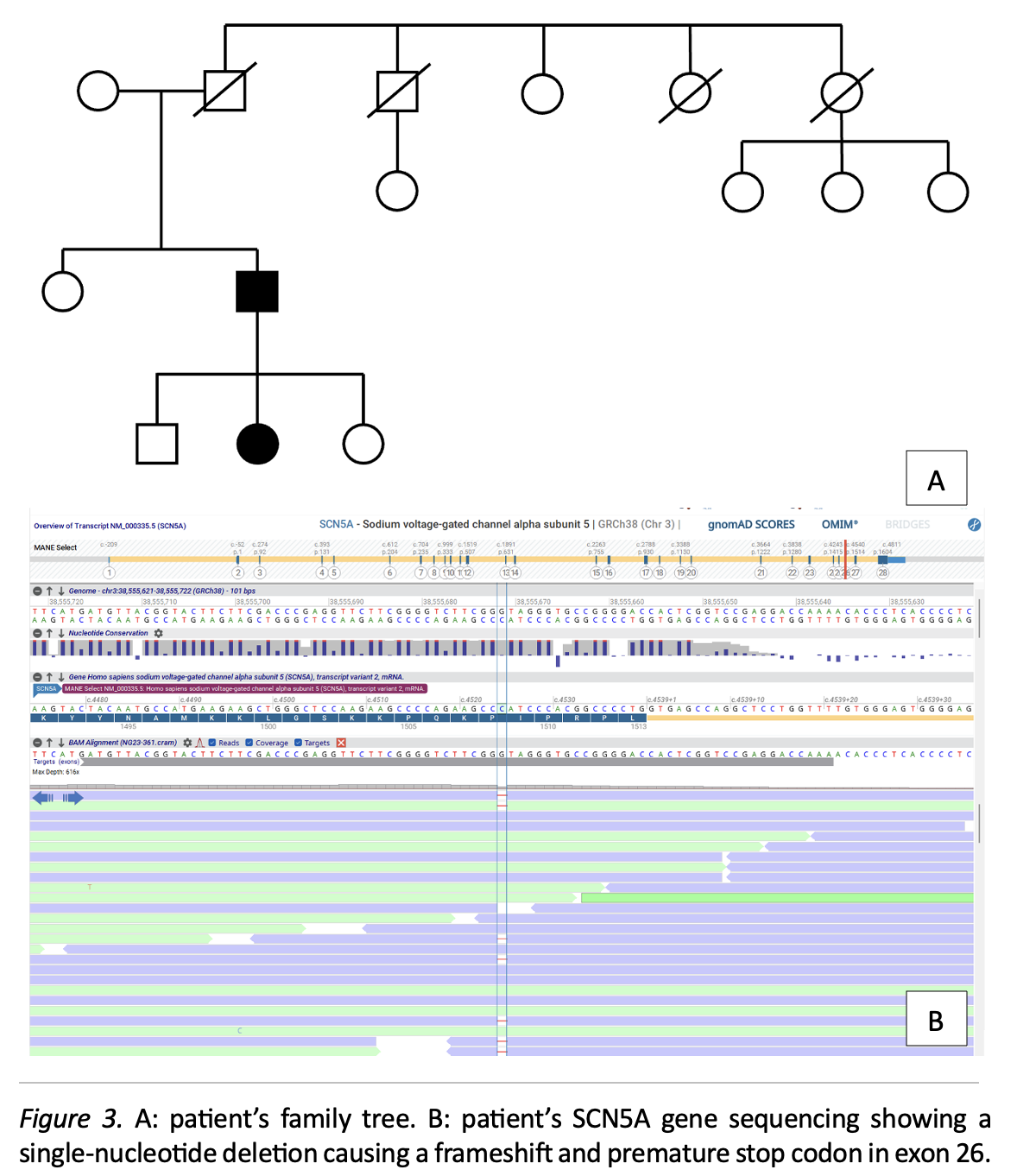
A 55-year-old Caucasian male presented to the emergency department for syncope. His past medical and familiar history was unremarkable. ECG showed sinus rhythm with Brugada-like V1-V2 pattern (no diagnostic type 1 pattern in standard and high intercostal leads). Laboratory tests, echocardiography, and chest X-ray were normal. Continuous ECG monitoring revealed intermittent left bundle branch block (LBBB), junctional bradycardia, and type 1 second-degree AV block. Coronary angiography excluded obstructive disease. Cardiac MRI showed normal findings. Electrophysiological study was negative for ventricular arrhythmia induction. The patient was discharged after loop recorder implantation. Subsequent genetic testing identified a heterozygous SCN5A mutation (p.Ile1510Serfs*5, previously unreported in literature), prompting a presumptive diagnosis of Brugada Syndrome (BrS). This variant involves a single-nucleotide deletion causing a frameshift and premature stop codon in exon 26, consistent with a loss-of-function mechanism. Two years later, another syncopal event occurred and a critical sinus atrial block (SAB, 8-second R-R interval) was documented. The clinical dilemma was whether to implant a pacemaker (indicated for symptomatic bradyarrhythmia) or an ICD (indicated for symptomatic BrS). Ajmaline challenge was performed under temporary transvenous pacing backup: the test was negative for type 1 Brugada pattern but induced worsening conduction abnormalities (LBBB, frequent sinus atrial blocks). BrS was excluded, and a dual-chamber pacemaker with left bundle branch area pacing was implanted for symptomatic SAB and progressive conduction disease. Family screening revealed the same SCN5A mutation in one of the patient’s children, with clinical and electrocardiographic investigations being negative. SCN5A mutations account for up to 20% of BrS cases but are also implicated in other phenotypes, including Long QT Syndrome type 3, cardiomyopathies, and conduction system disease (CSD). Overlap syndromes pose significant diagnostic challenges, but BrS diagnosis remains primarily clinical and ECG-based rather than genetic. SCN5A-related BrS and CSD share a common pathophysiological substrate, with phenotypic expression likely depending on complex interactions between SCN5A and other regulatory factors rather than the degree of current reduction alone. Integrating clinical, genomic, and proteomic data is essential to unravel the complexity of SCN5A-related conditions.