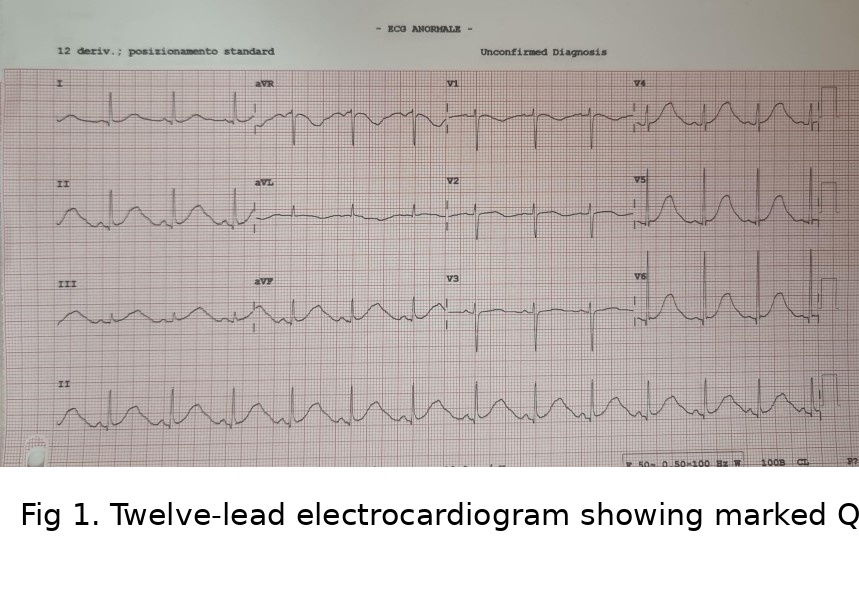
We present the case of a 31-year-old woman, affected by congenital long QT syndrome (LQTS) diagnosed at ten weeks of pregnancy. Family history showed a case of sudden cardiac death (SCD): a paternal uncle died suddenly at the age of 40 years. The patient had experienced recurrent episodes of syncope since adolescence, incorrectly labeled as absence-type epilectic seizure and treated with lamotrigine for many years, with no benefits. Syncope events were frequently triggered by acoustic stimuli, particularly during early morning hours, followed by autonomic symptoms including palpitations and vomiting. Patient was admitted to our cardiology department on 15 th July 2025 for recurrent syncope and chest discomfort. ECG revealed marked QT prolongation (QT 628 ms, QTc 540 ms, RR 740 ms) with abnormal T-wave morphology (Figure 1). For confirmation of LQTS, patient underwent genetic testing in a tertiary center. Awaiting the test results (almost two months), patient was treated with nadolol 40 mg daily and discharged with a wearable cardioverter-defibrillator (Life Vest, Zoll) as a temporary protective measure. After two months, genetic test confirmed LQT2 syndrome, based on a mutation in gene KCNH2. Given the history of recurrent syncope, marked QTc prolongation ≥ 500 ms and a family history of SCD, the patient was scheduled for subcutaneous ICD (S-ICD) implantation, as primary prevention. In the context of ongoing pregnancy, X-ray and general anesthesia were not used during S-ICD implantation. Under regional anesthesia with ultrasound-guided serratus anterior plane block and parasternal block, Emblem S-ICD (Boston Scientific) was successfully implanted with no peri-procedural complications (Figure 2). Shock impedance was 80 Ohm. Post-procedural maternal and fetal courses were uneventful (Figure 3) and patient was discharged after 3 days on nadolol, with planned multidisciplinary follow-up. After 6 months of follow up, patient was asymptomatic, any arrhythmic events were recorded and pregnancy was progressing well in the third trimester. LQTS is a potentially life-threatening inherited arrhythmia disorder, with risk of malignant ventricular arrhythmias during specific physiological conditions, including pregnancy and the postpartum period. This case highlights several clinically relevant aspects: diagnostic delay of LQTS due to misinterpretation of symptoms, LQTS risk stratification in pregnancy and feasibility of fluoroscopy-free subcutaneous ICD implantation.