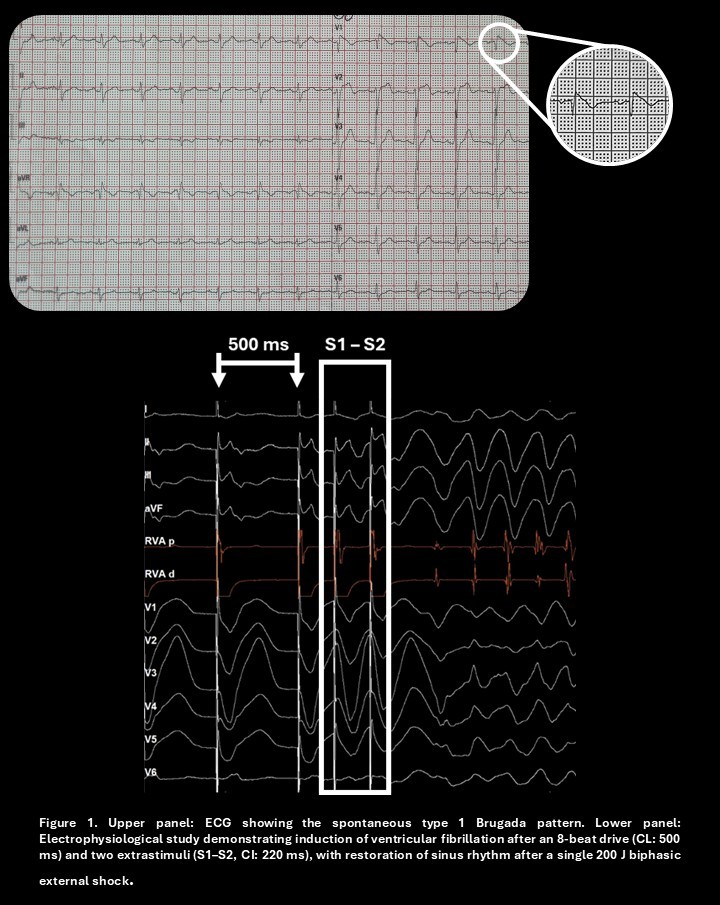
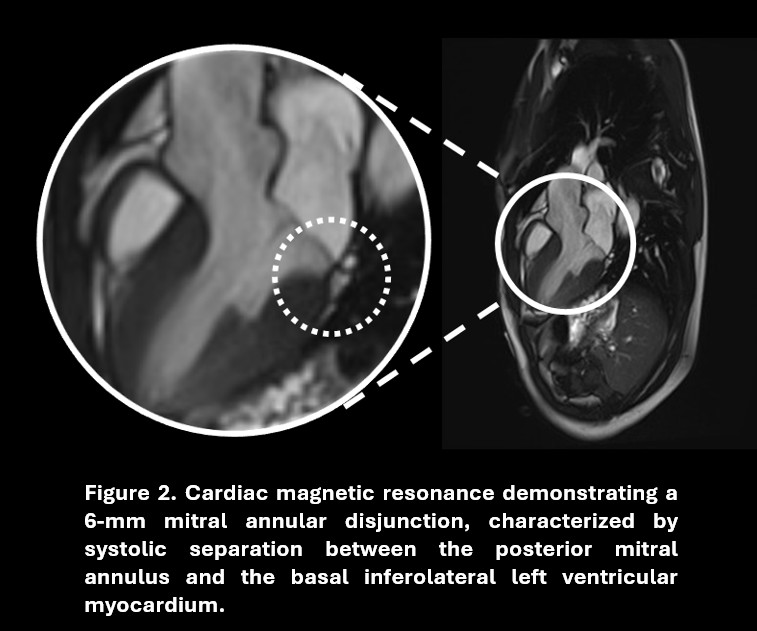
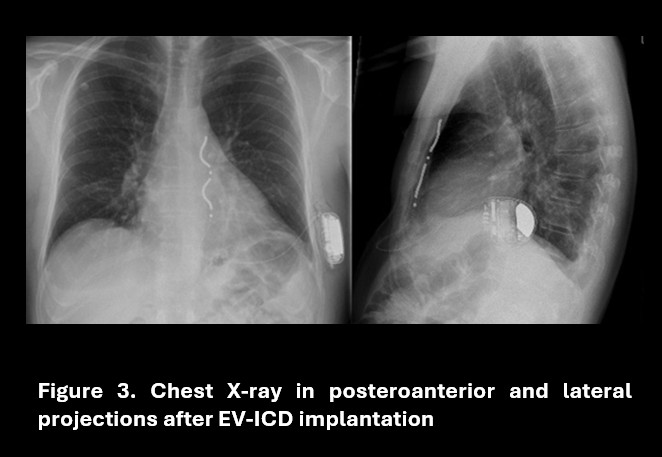
A 34-year-old woman with a known spontaneous type 1 Brugada ECG pattern presented to the emergency department after a syncopal episode. Her medical history included a likely pathogenic SCN5A gene variant (with both her father and son affected) and a family history of sudden cardiac death. She was admitted for arrhythmic risk stratification. Transthoracic echocardiography showed only mild atrioventricular valve regurgitation. According to the 2022 ESC Guidelines on ventricular arrhythmias and sudden cardiac death prevention, an electrophysiological study was performed. Using a drive cycle length of 500 ms and double extrastimuli at 220 ms, ventricular fibrillation was induced and terminated by a single external 200 J DC shock. The patient was therefore considered for defibrillator implantation, preceded by cardiac magnetic resonance (CMR) for morpho-tissue characterization. CMR revealed mild mitral regurgitation due to redundant, prolapsing mitral leaflets, associated with mitral annular disjunction (MAD) of 6 mm, systolic curling of the basal inferolateral and anterolateral left ventricular segments, and late gadolinium enhancement (LGE) involving the posteromedial papillary muscle. In addition, tricuspid annular disjunction (TAD) of 4 mm was observed. These findings complicated attribution of the arrhythmic substrate to either the channelopathy or the mitral valve disease. MAD is a structural abnormality frequently associated with mitral valve prolapse, with a reported prevalence of up to 40%. A MAD ≥5 mm has been linked to an increased risk of ventricular arrhythmias, particularly in the presence of myocardial fibrosis. The coexistence of MAD, systolic curling, and LGE defines a high-risk arrhythmic phenotype with important implications for risk stratification and management. Given the patient’s young age and the absence of pacing indications, an extravascular ICD (EV-ICD) was implanted, allowing post-shock pacing and antitachycardia pacing while avoiding intravascular components and reducing infection risk. In conclusion, this case highlights the complexity of arrhythmic risk stratification, suggesting the coexistence of distinct but potentially synergistic arrhythmogenic substrates, and supports a multiparametric approach integrating genetics and advanced cardiac magnetic resonance imaging, aimed at optimizing therapeutic management and guiding the selection of the most appropriate implantable defibrillator