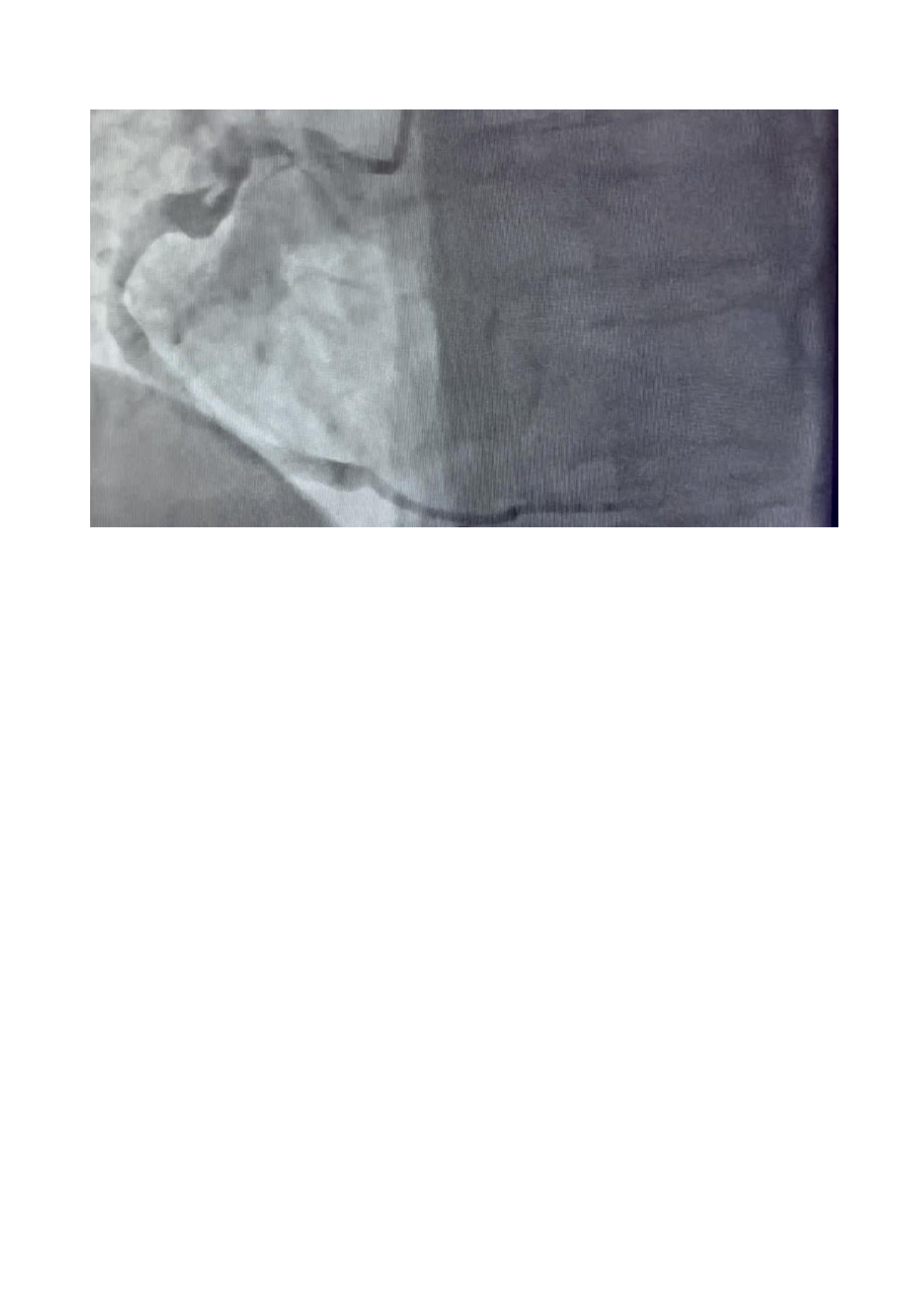
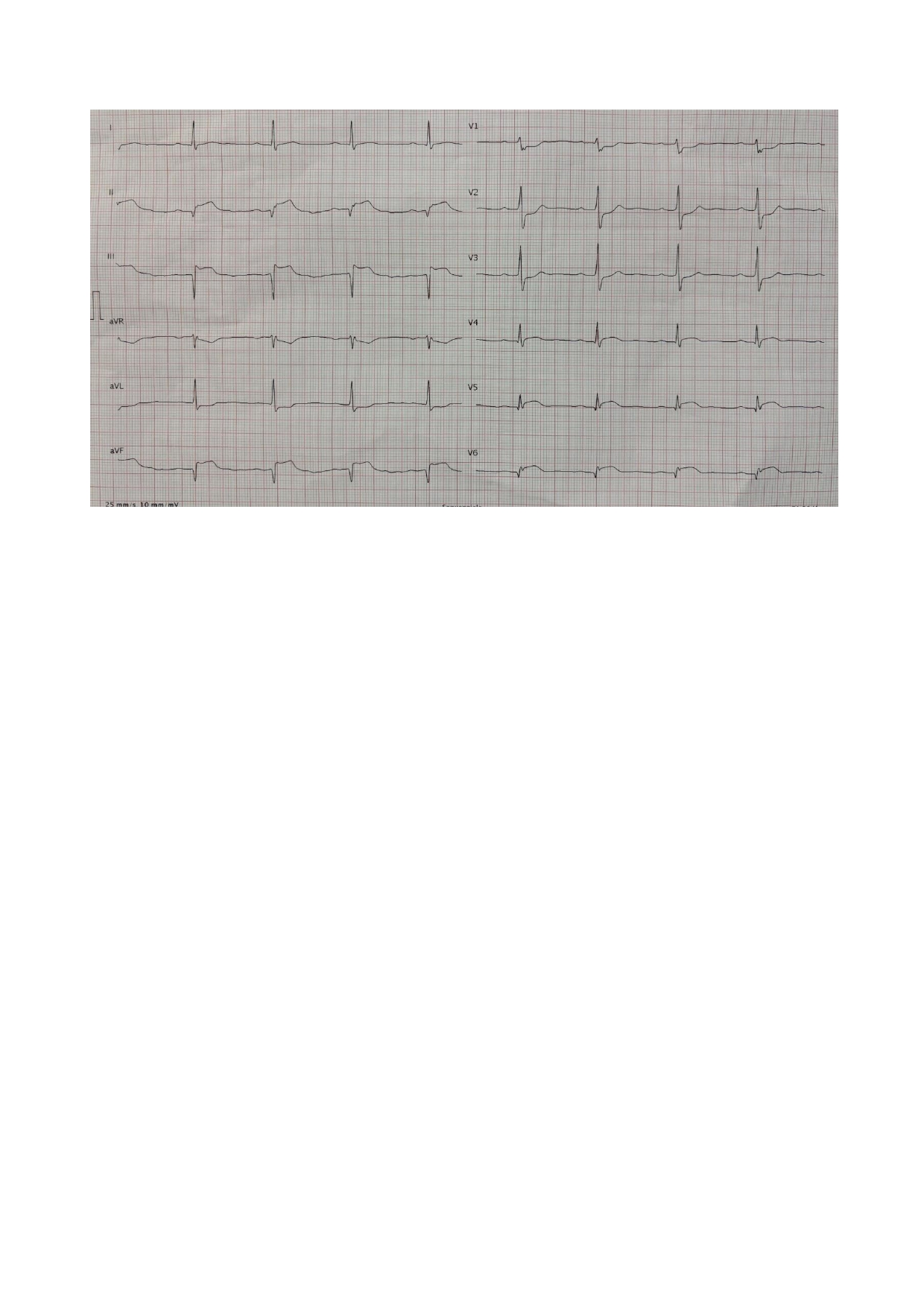
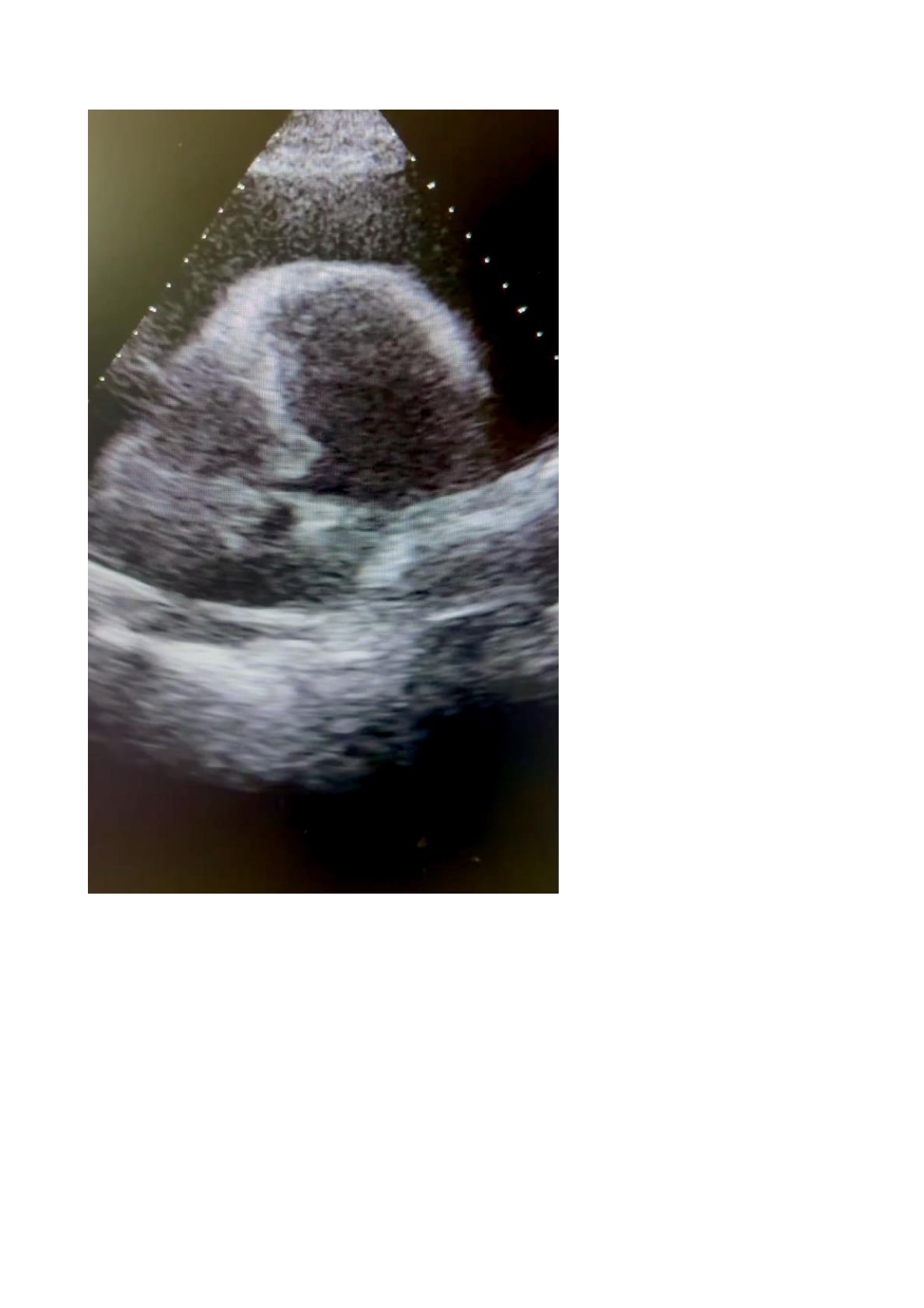
Background: Dressler’ssyndrome, a rare post-infarctioninflammatorycomplication in the era of earlymechanicalreperfusion, mayoccurseveral days after the acute ischemic event. We report a case of infero-lateral STEMI complicated by no-reflow and subsequentpleuro-pericardialeffusion, successfullymanagedthrough a multidisciplinaryapproach. Case Presentation: A 66-year-old obese, hypertensive man in good therapeutic control presented with chestpainduringexertion. ECG showed an evolved infero-lateral STEMI. Echocardiographyrevealed an ejectionfraction (EF) of 30% with infero-posterolateralakinesia. Urgentcoronaryangiographydemonstrateddiffuselyatheromatous vessels and a rightcoronaryartery (RCA) with muralaneurysms and TIMI 1–2 flow. PCI with drug-elutingstentimplantation on the distal RCA wasperformed. No-reflowoccurred and wastreated with intracoronary adenosine and tirofibaninfusion. The coursewascomplicated by intermittent second-degree AV block (2:1) and a circumferentialpericardialeffusion (28 mm) with earlyright-sidedcompression, treated with colchicine, NSAIDs, and pericardiocentesis (900 mL of citro-hematicexudate). Bilateralpleuraleffusion (55 mm on the left one) wasdrained (2 L of citrine fluid). Discussion: This case underscores the complexity of post-STEMI evolutioneven in the reperfusion era. The coexistence of no-reflow, conductiondisturbances, and Dressler’ssyndromerequiresvigilant monitoring and prompt, coordinated management of inflammatory and mechanicalcomplications. Early use of colchicine, NSAIDs, and drainage led to resolution of effusions and hemodynamicstabilization. Conclusions: Although rare, Dressler’ssyndromeremains a possible late inflammatoryevolution after STEMI. Earlyrecognition and integrated treatment allowed clinical improvement and partial recovery of leftventricularfunction (EF 37% atdischarge).