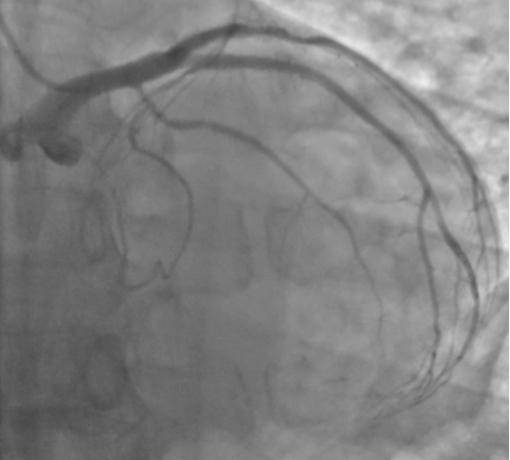
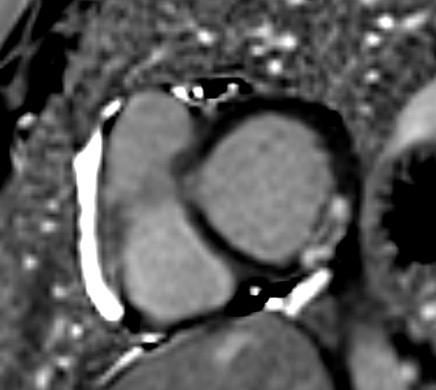
A 41-year-old man with a history of prior anterior myocardial infarction (MI), previously treated with primary percutaneous coronary intervention (PCI) of the left anterior descending artery (LAD) and staged PCI of the left circumflex (LCx) and right coronary artery, was admitted for sudden left-sided paraesthesia. Blood tests revealed marked myocardial injury (peak high-sensitivity troponin 21,931 ng/mL), and ECG showed silent ischemic changes. Transthoracic echocardiography demonstrated chronic apical akinesia with a newly detected, round, homogenous hyperechoic apical thrombus measuring 10 mm (Fig. 3). Given the risk of haemorrhagic transformation while on triple antithrombotic therapy [1]—and in the absence of clinical instability—coronary angiography was deferred. Initial head CT was unremarkable; however, brain MRI performed the following day revealed a large right occipito-mesial infarction with ipsilateral thalamic involvement. Anticoagulation with adjusted-dose low molecular weight heparin (LMWH) was initiated in agreement with neurology. Follow-up CT at day 5 excluded haemorrhagic conversion. Cardiac magnetic resonance imaging confirmed a minute apical thrombus and demonstrated an acute basal posterior myocardial infarction with microvascular obstruction (Fig. 2). Subsequent coronary angiography revealed chronic LAD stent occlusion with patency of previously implanted LCx and RCA stents (Fig. 1). Overall, the findings were consistent with myocardial infarction with non-obstructive coronary arteries (MINOCA), most likely of cardioembolic origin [2]. The patient was discharged with neurological improvement on aspirin and therapeutic LMWH, with transition to oral anticoagulation planned after 1-month CT reassessment. Simultaneous cardioembolic stroke and MINOCA remain a rarely reported association. This case highlights the importance of considering an embolic mechanism in patients presenting with neurological symptoms and evidence of myocardial ischemia. Multimodality imaging improved diagnostic accuracy. Management was particularly challenging because the need for anticoagulation coexisted with the risk of haemorrhagic transformation. The decision to postpone coronary angiography, guided by symptoms, proved appropriate.