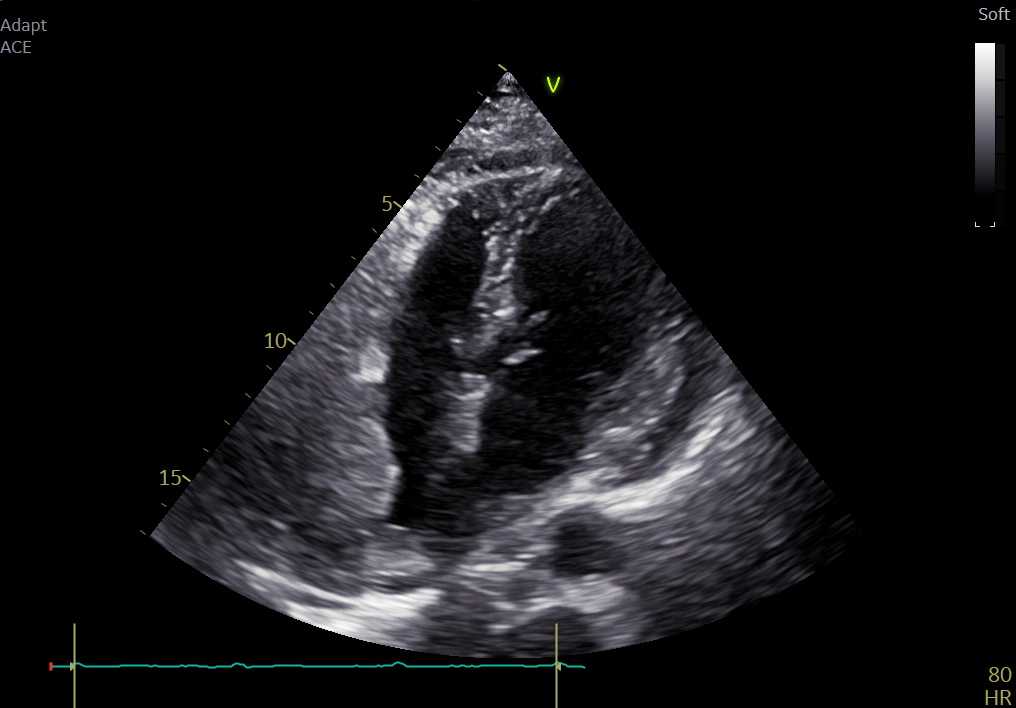
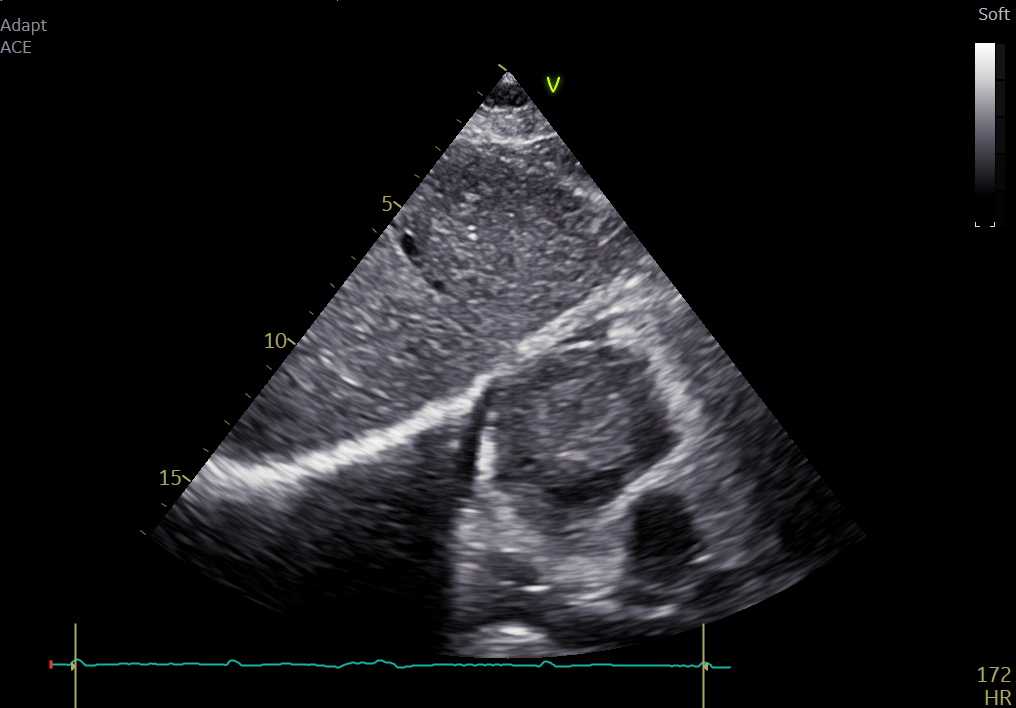
Cardiac angiosarcoma is a malignant tumor of the heart, usually located in the right atrium, originating from the endothelial lining of the vessels and infiltrating the surrounding myocardium. A 70-year-old woman was admitted to our emergency department with dyspnea and palpitations. A 12-lead electrocardiogram revealed atrial flutter, successfully treated with electrical cardioversion, and oral anticoagulation was initiated. Transthoracic echocardiography showed a trivial circumferential pericardial effusion and a marked thickening of the right atrial free wall, mimicking a large mass (Fig.1, fig. 2). CT confirmed a giant mass (57×46×65 mm) in the right atrial wall, hypodense with areas of intense vascularization becoming hyperdense after contrast injection. Abdominal CT revealed multiple small hypodense liver lesions and mesenteric involvement, while FDG-PET showed increased glucose uptake only in the atrial mass. Cardiac MRI demonstrated infiltration of the right atrial free wall, extension to the right atrioventricular sulcus with thight adherence to the right coronary artery and extension to the cranial portion of the right ventricle, with a hypovascularized core and patchy late gadolinium enhancement. After a non-diagnostic liver biopsy, a direct right atrial biopsy was performed, leading to the definitive diagnosis of conventional angiosarcoma. Following this challenging diagnosis, the patient was referred to the Oncology Department and started appropriate chemotherapy.