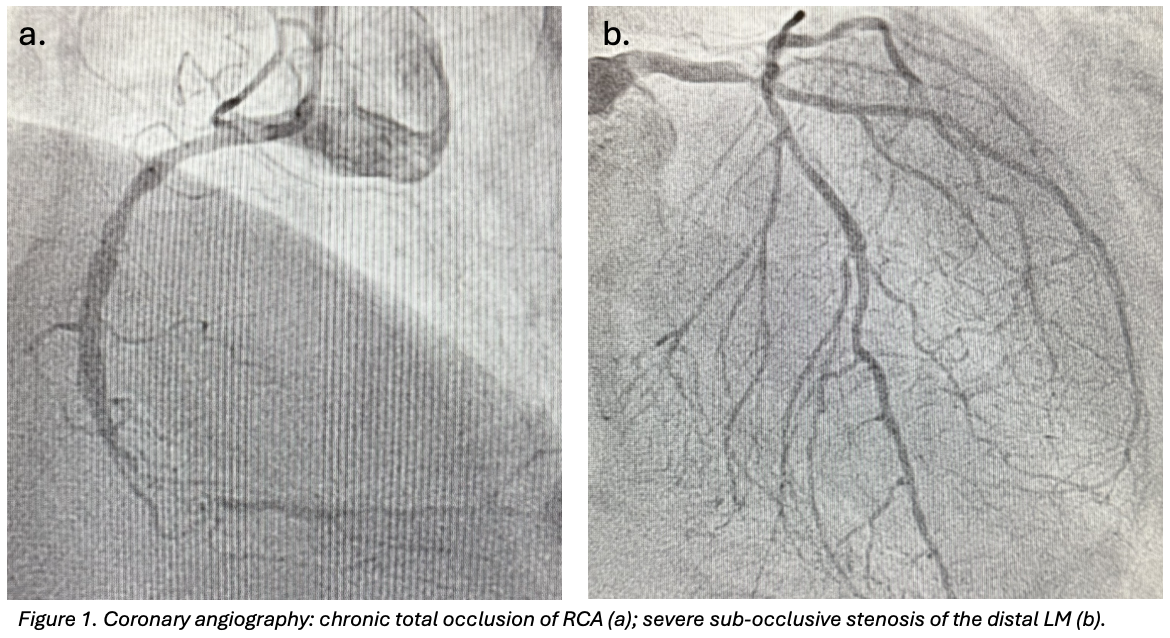
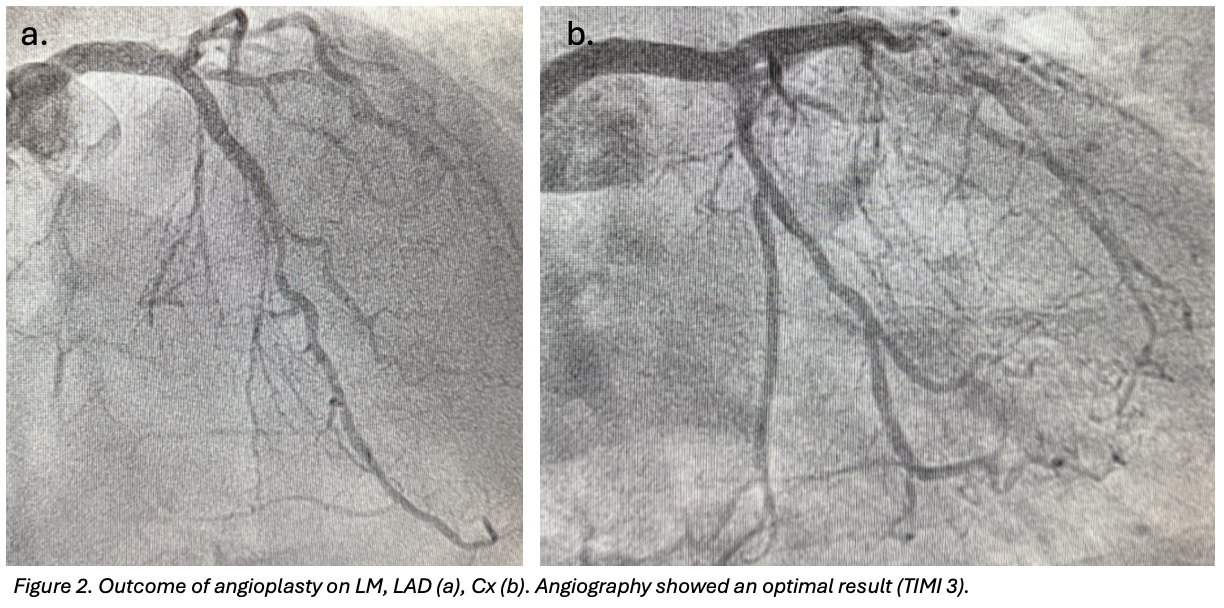
CLINICAL CASE A 77-year-old man was admitted to the Emergency Department with a two-hour history of chest pain and recurrent angina over the previous month. Physical examination and vital signs were unremarkable. EKG showed diffuse ventricular repolarization abnormalities and TnT was 1,200ng/L. Transthoracic echocardiography revealed preserved biventricular systolic function. Medical history included anterior STEMI treated with PCI on the left anterior descending artery (LAD) in 2012, chronic total occlusion of the right coronary artery (RCA), peripheral artery disease. Cardiovascular risk factors were arterial hypertension, diabetes mellitus II, dyslipidaemia. A diagnosis of NSTEMI was made. MANAGMENT Coronary angiography demonstrated a good angiographic result of the previous PCI and a severe sub-occlusive stenosis of the distal LM (fig.1). PCI of the LM was performed under mechanical circulatory support with an intra-aortic balloon pump (IABP). The left coronary system was engaged with a 7F XB 3 guiding catheter, with guidewires positioned in the LAD and protective wires in the circumflex artery and intermediate branch. After lesion preparation on LM with a semi-compliant balloon, plaque modification was achieved using intravascular lithotripsy (IVL, Shockwave system) due to severe calcification. A 3.5×34mm drug-eluting stent was implanted from LM to proximal LAD in overlap with the previous stent. Repeated kissing balloon inflations and final proximal optimization technique (POT) were performed. The circumflex artery was treated with a 3×15mm drug-coated balloon, followed by final kissing balloon inflation. Final angiography showed an optimal result (TIMI 3 flow) and no complications (fig.2). The IABP was removed at the end of the procedure. OUTCOME AND FOLLOW-UP The in-hospital course was uneventful, with no arrhythmic events. At one-month follow-up, the patient was asymptomatic with no anginal recurrence. FUTURE PERSPECTIVES Timely revascularization of critical LM disease is crucial, particularly in high-risk patients. Mechanical circulatory support with IABP may provide additional safety during complex LM PCI. IVL represents a valuable calcium debulking device, allowing effective lesion preparation with a safety profile (low risk of dissection, perforation, distal embolization. Finally, meticulous bifurcation technique, including final POT, plays a crucial role in optimizing stent expansion and long-term outcomes.