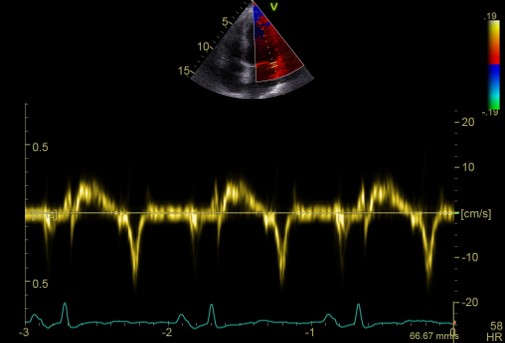
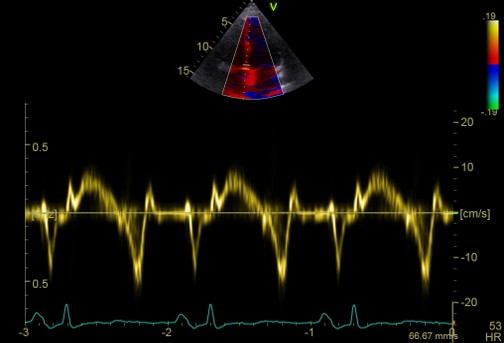
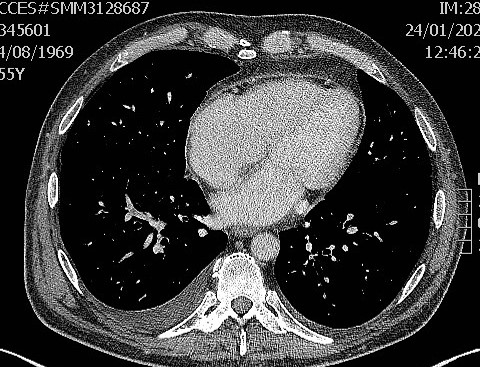
INTRODUCTION: Constrictive pericarditis is a pericardial syndrome characterized by pericardial rigidity, with possible thickening and calcification, leading to impaired diastolic filling. CASE REPORT: A 55-year-old man with a medical history of systemic arterial hypertension, active smoking, previous cocaine abuse, and seropositive rheumatoid arthritis. The patient had been complaining of exertional dyspnea for approximately two years. In 2023, he was admitted to the Cardiology Department for chest pain; coronary angiography showed normal coronary arteries, while cardiac magnetic resonance imaging revealed thickened pericardial layers, pericardial edema, and constrictive physiology. In the following months, he was rehospitalized for signs and symptoms of right-sided heart failure, and low-dose furosemide therapy was initiated. In January 2025, the patient was admitted again for worsening exertional dyspnea (NYHA class III). Physical examination revealed jugular venous distension, hepatomegaly, pulsus paradoxus, positive hepatojugular reflux and peripheral edema. Laboratory tests showed elevated cholestatic indices and transaminases and low NT-proBNP levels. Transthoracic echocardiography demonstrated preserved left ventricular systolic function, normal valvular morphology and function, abnormal interventricular septal motion (septal bounce), marked respiratory variation of the mitral E-wave, ventricular interdependence, and an inverted medial-to-lateral e′ ratio (annulus paradoxus). Cardiac catheterization revealed equalization of ventricular end-diastolic pressures during inspiration and a “dip-and-plateau” pattern of right ventricular pressure. Contrast-enhanced cardiac computed tomography confirmed constrictive physiology and pericardial thickening. The case was discussed with the Rheumatology team, who hypothesized an association between rheumatoid arthritis and constrictive pericarditis. The patient was therefore referred for cardiothoracic surgical evaluation, and pericardiectomy was indicated. After surgery, the patient remained clinically and laboratoristically stable. CONCLUSIONS: Constrictive pericarditis should be suspected in the presence of systemic congestion signs and symptoms, NT-proBNP levels disproportionally low relative to the degree of congestion, and a normal first-level echocardiographic assessment; particularly in patients with a history of recurrent pericarditis, systemic inflammatory diseases, or prior chest radiotherapy.