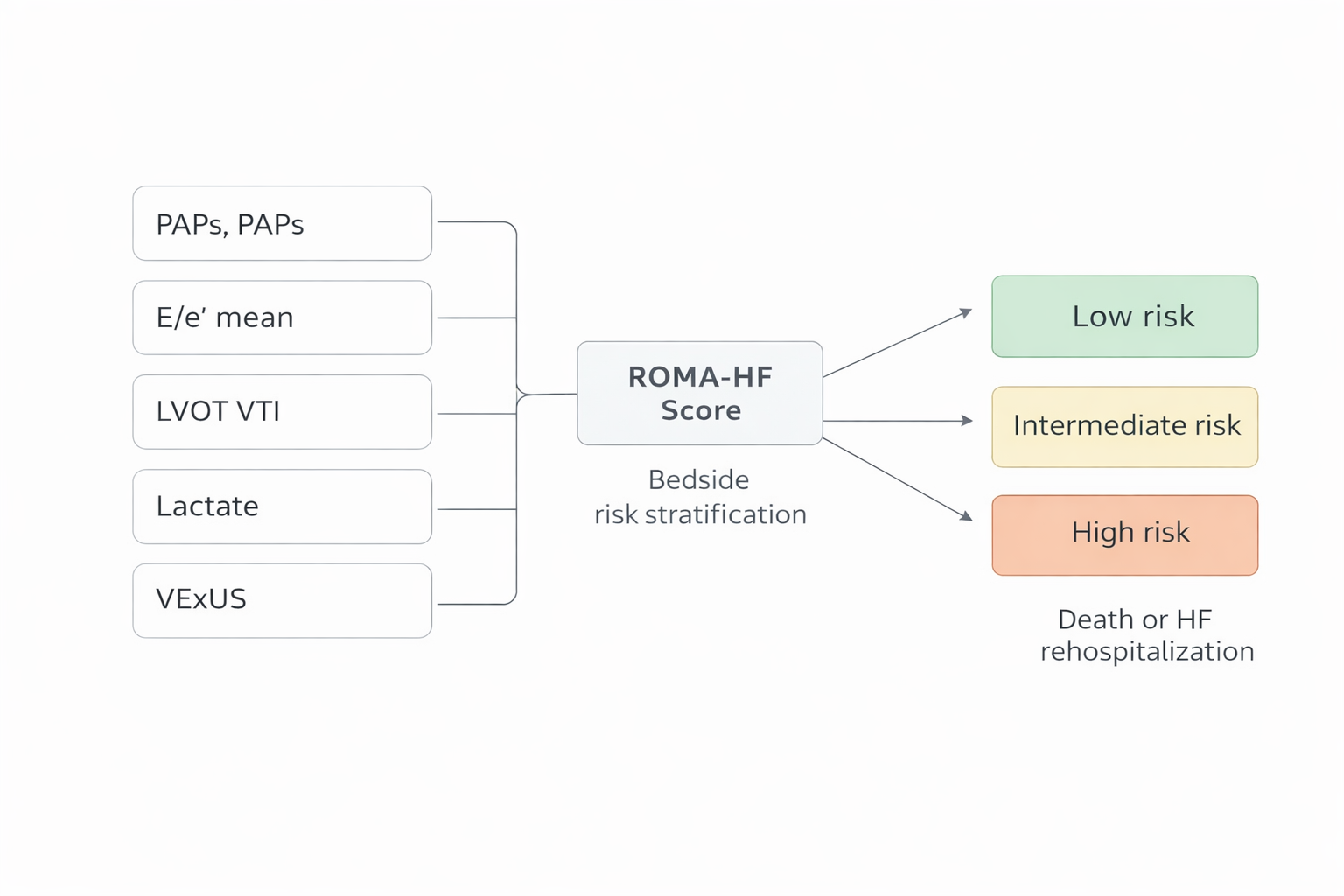
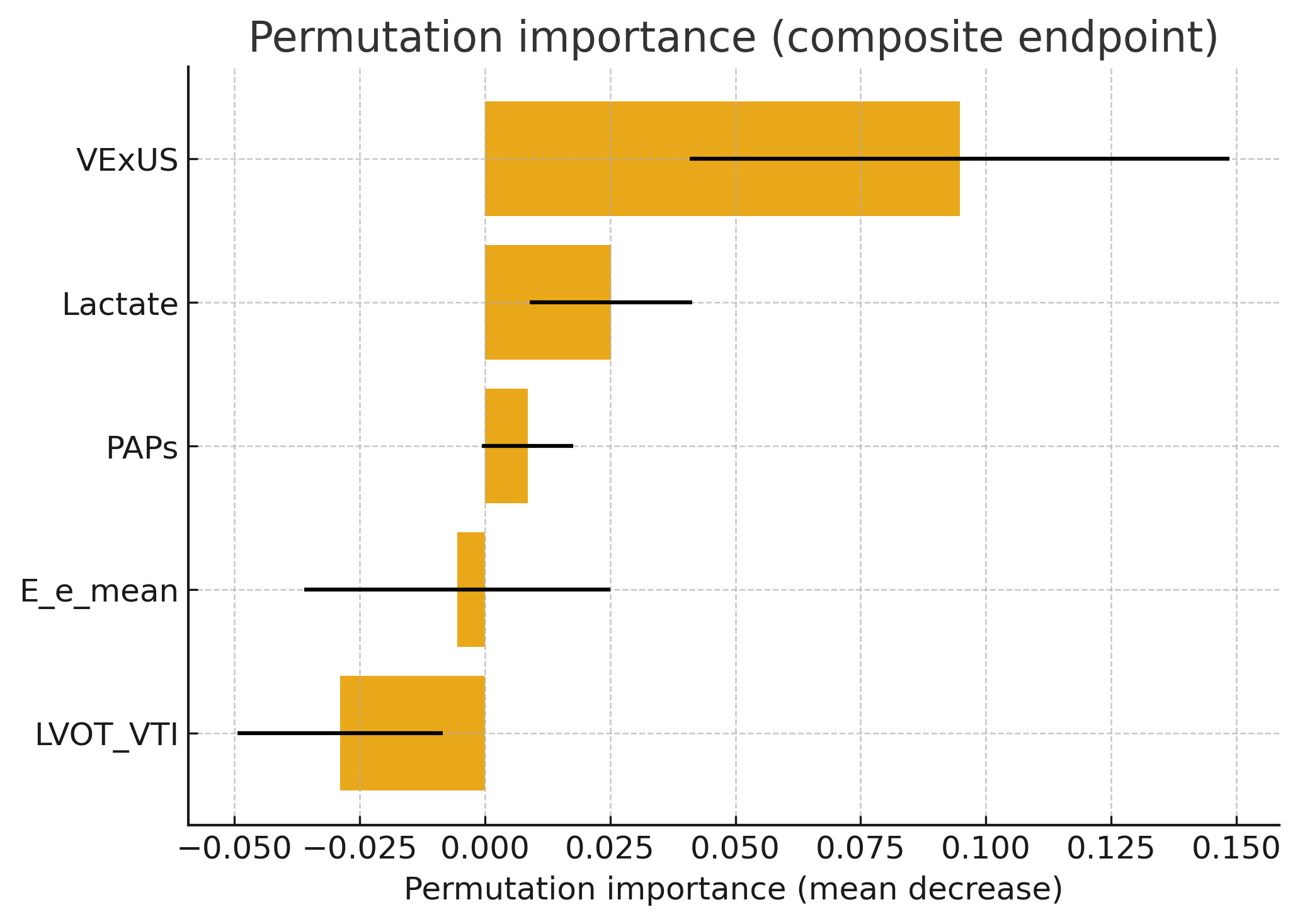
Background Risk stratification in patients with acute heart failure(AHF) remains challenging. Many available prognostic models rely on complex variables or are poorly applicable at the bedside and do not adequately capture the pathophysiological role of systemic congestion and metabolic impairment, which are key drivers of adverse outcomes. Methods A pragmatic bedside risk model was developed(ROMA HF: Risk Of Major Adverse events in Heart Failure)integrating five readily available variables reflecting congestion and metabolism: systolic pulmonary arterial pressure, mean E/e′ ratio, left ventricular outflow tract velocity–time integral, blood lactate, and venous excess ultrasound score(VEXUS). The model was tested in 62 consecutive patients hospitalized for AHF. Logistic regression was used to estimate individual risk for a composite endpoint of all-cause mortality or heart failure rehospitalization. Patients were stratified into tertiles of predicted risk. Model discrimination was assessed using area under the ROC curve with bootstrap validation. Survival analyses were performed using Kaplan–Meier curves. Variable relevance was explored using permutation importance and penalized regression models. Results During follow-up, 41/62 (66%) patients experienced the composite endpoint (19/62 deaths, 31%; 22/62 HF rehospitalizations, 35%). Event rates increased across risk tertiles: 19% (low), 30% (intermediate), and 67% (high). Discrimination was good for the composite endpoint (AUC 0.78), and remained consistent for mortality (AUC 0.75) and rehospitalization (AUC 0.72). In permutation importance, the strongest contributors were VExUS (0.095 ± 0.054) and lactate (0.025 ± 0.016), followed by PAPs (0.009 ± 0.009). Penalized models confirmed congestion-related dominance: LASSO retained VExUS (β=0.45) and E/e′ mean (β=0.11), while Elastic Net emphasized VExUS (β=0.51) and E/e′ mean (β=0.20). Conclusions A simple bedside model integrating congestion and metabolic parameters allows effective prognostic stratification in acute heart failure. This approach may support clinical decision-making and prioritization of care pathways in high-risk patients.