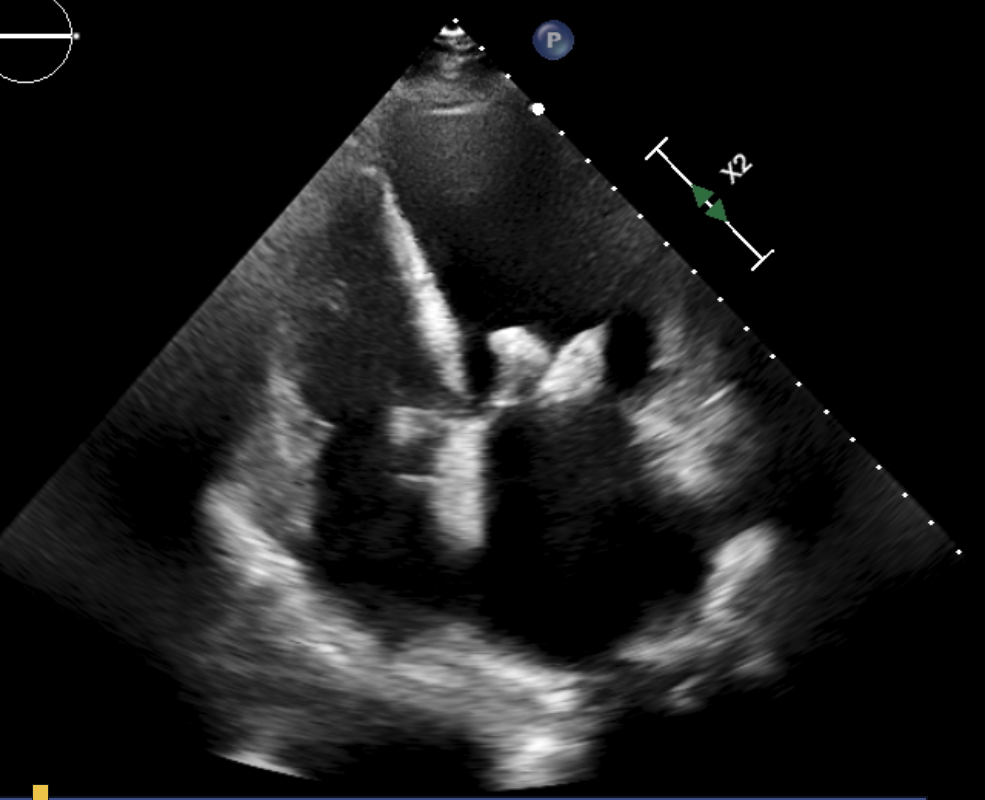
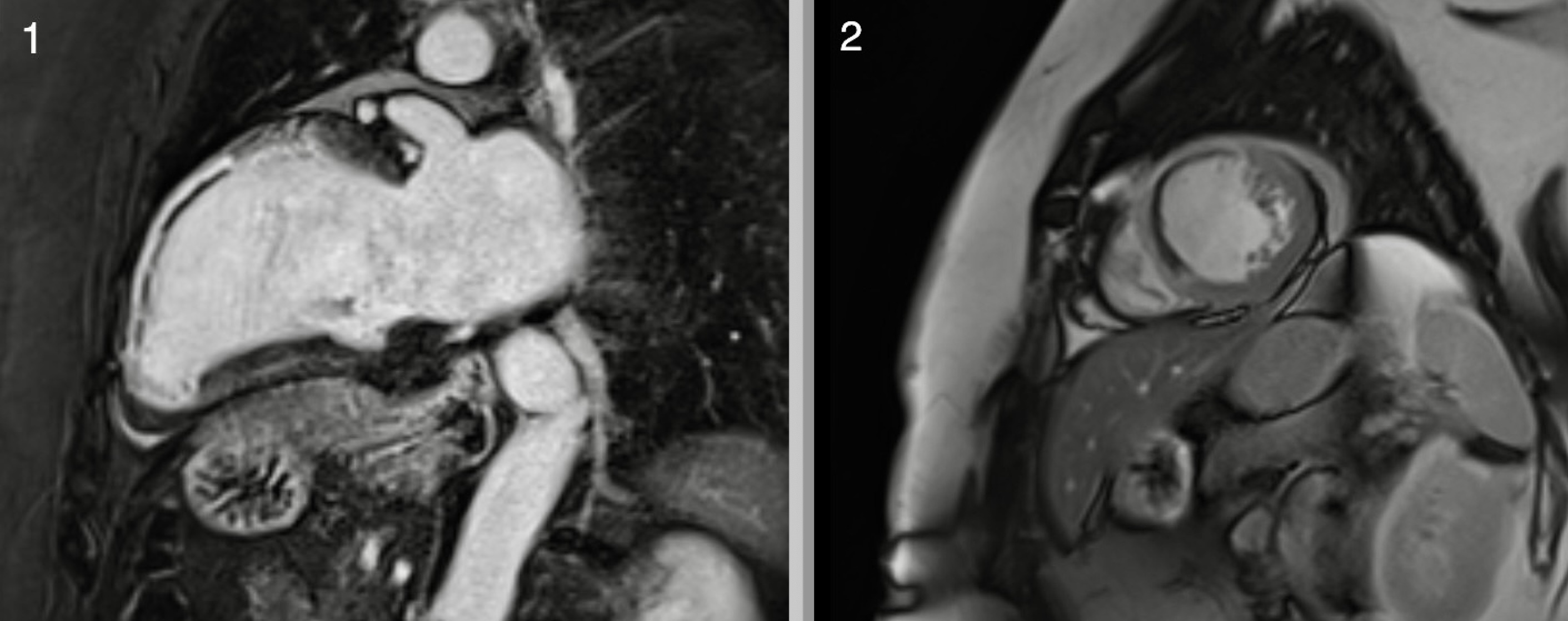
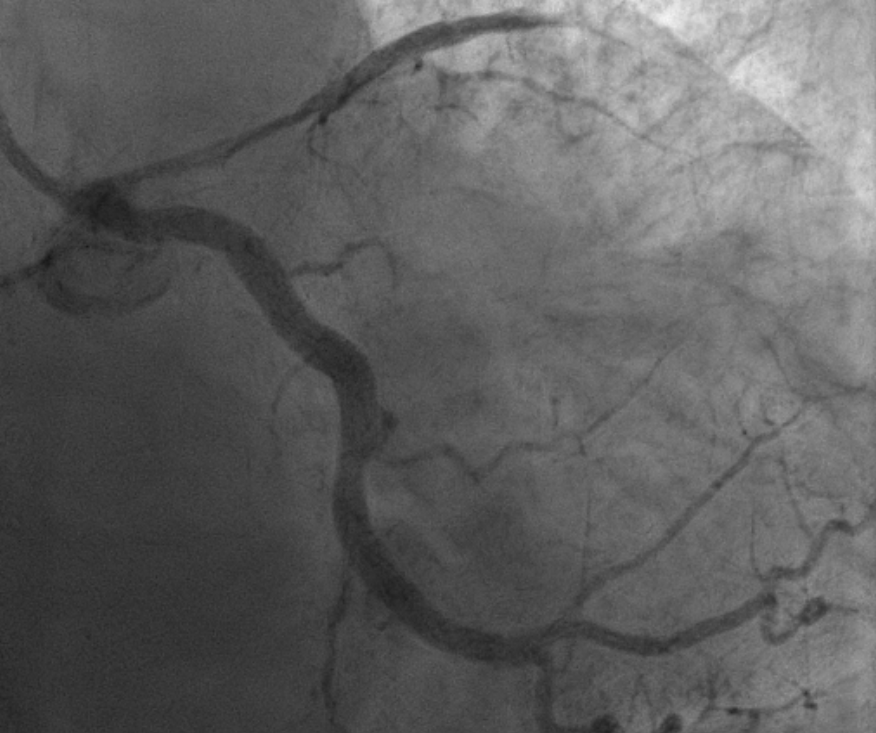
A 63-year-old woman was admitted to Padova University Hospital for STEMI after seeking medical help for typical chest pain. The initial EKG showed a left bundle branch block with significant ST-segment elevation from V2 to V4. After a short pain to balloon time (< 2 hours), she underwent coronary angiography, which showed critical thrombotic stenosis (85%, TIMI 1) of the proximal LAD, treated with double DES; transient slow-flow was treated with adenosine and verapamil; the final TIMI flow was 2. The pre-discharge LVEF was 37%. Eight days after the acute event, cardiac MRI revealed severely reduced LVEF (33%) due to dyskinesia of the apex and akinesia of the whole LAD territory. TIRM sequences showed transmural edema in the same areas; corresponding transmural LGE (ischemic pattern) and dark zone referring to microvascular haemorrhagic damage was noted. Given the extent and severity of myocardial damage despite the short pain-to-balloon time, microvascular obstruction was hypothesized. Due to enrolment in a research project, functional autoantibodies (AAs) targeting angiotensin II receptor type 1 (AT1R) and endothelin-1 receptor type A (ETAR) were measured, showing significantly high levels (ETAR-AAs 11,12 U/mL and AT1R-AAs 10,87 U/mL, with the cutoff for seropositivity being >10 U/mL). Due to multiple episodes of decompensated heart failure, CRT-D was implanted, and double mitral TEER was performed with limited efficacy. Right heart catheterization confirmed combined pre- and post-capillary pulmonary hypertension and severe reduction of cardiac index (1,75 l/min/m 2 ). After a multidisciplinary discussion, the transplantation process was initiated. HLA panel exhibited high immunogenicity, and the calculated Panel Reactive Antibodies (cPRA) was 92%, reducing the chances of finding a suitable organ. Desensitization therapy with plasmapheresis and rituximab was initiated. In July 2025, she underwent orthotopic heart transplantation. Two endomyocardial biopsies of the graft showed the absence of rejection, confirming the effectiveness of the anti-rejection therapy implemented before and after transplantation. This case shows how an autoimmune profile (including high AT1R-AAs and ETAR-AAs levels) can affect prognosis and transplantation after an acute coronary syndrome. Nonetheless, immunomodulation can help reduce the risk of graft rejection.