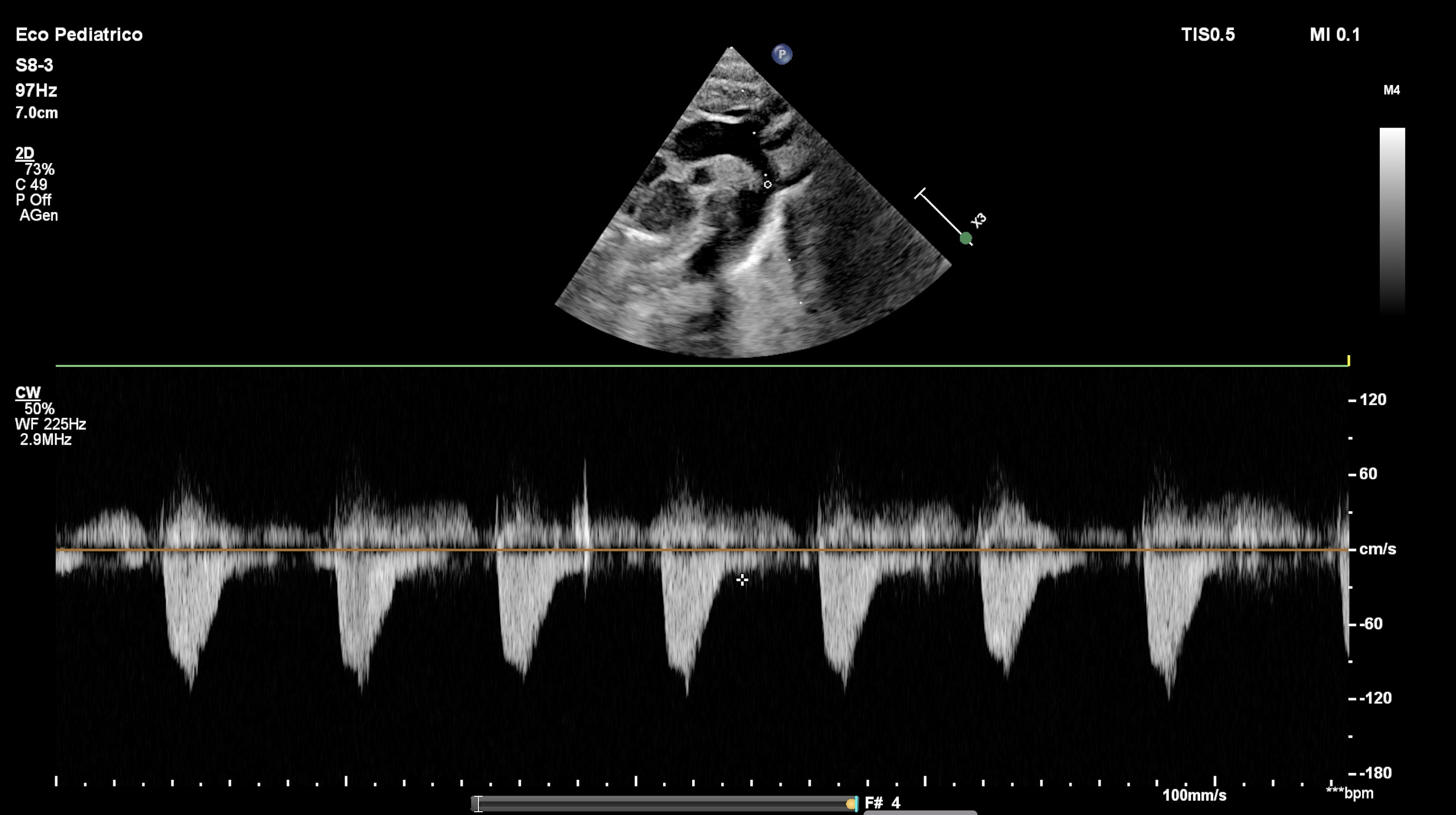
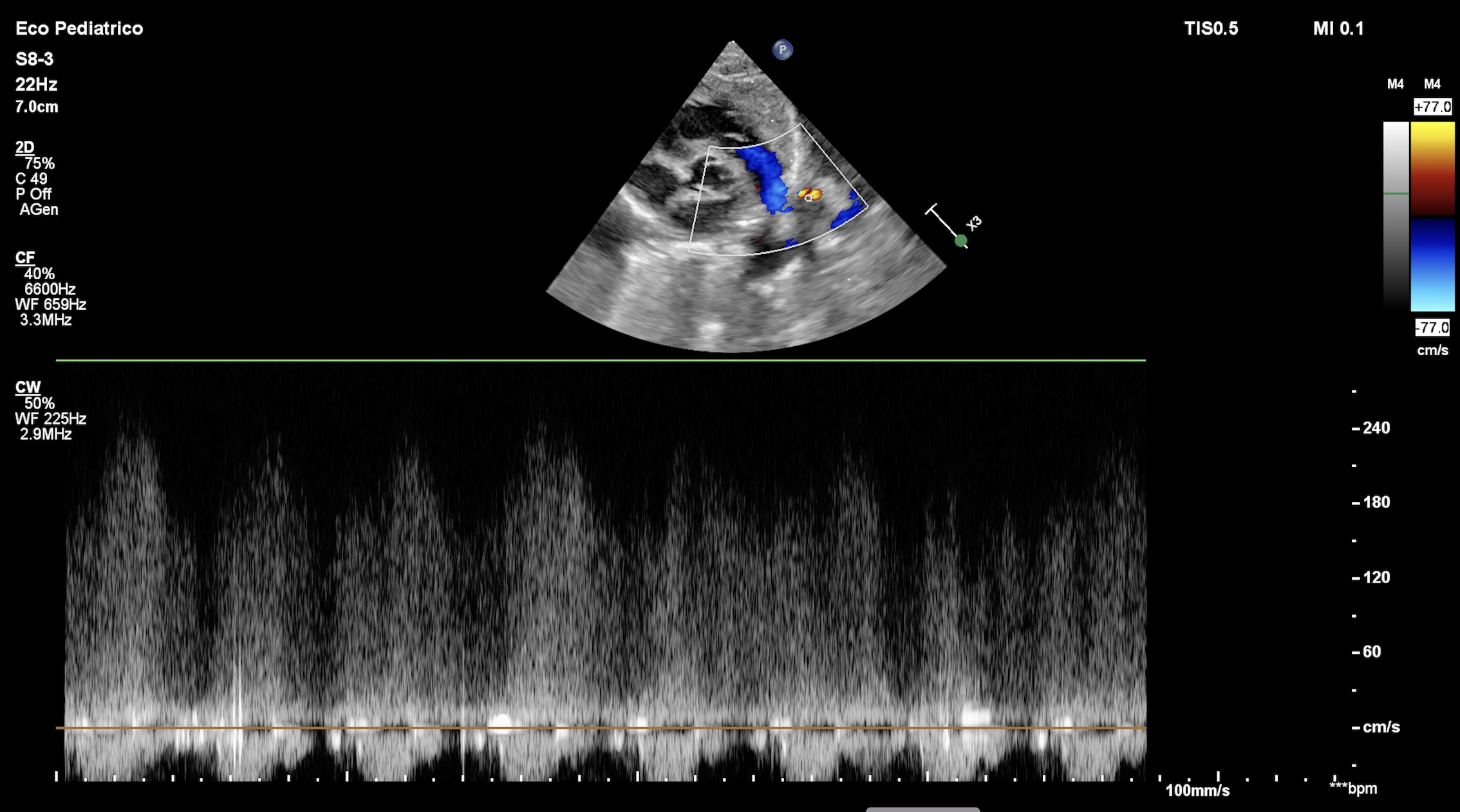
Background: Aortic coarctation is a critical congenital heart disease that may present in the neonatal period, often requiring urgent intervention. However, transitional cardiovascular changes after birth, particularly involving the ductus arteriosus, may mimic its echocardiographic features. Clinical case: A male neonate was born at 39+2 weeks of gestation via spontaneous vaginal delivery after an uneventful pregnancy. The infant was clinically stable and admitted to the postnatal ward. At 36 hours of life, a routine physical examination revealed a soft systolic murmur at the left upper sternal border. Peripheral pulses were palpable and symmetrical, and oxygen saturation was 98% in both pre- and post-ductal measurements. Blood pressure measurements showed a mild difference between upper and lower limbs. Transthoracic echocardiography demonstrated mild narrowing of the aortic isthmus without a clear indentation (“shelf”), turbulent flow at the juxtaductal region and a peak systolic gradient of approximately 20 mmHg, raising suspicion of aortic coarctation. The ductus arteriosus appeared small with high-velocity left-to-right flow, suggesting ongoing closure. Left ventricular function was normal, and no other structural cardiac anomalies were identified. Given the echocardiographic findings, the infant was transferred to a tertiary neonatal cardiology unit for further evaluation. PGE1 infusion was considered but withheld due to the infant’s stable clinical condition. Serial echocardiographic assessments were performed over the following 72 hours. Progressive complete closure of the ductus arteriosus was observed, accompanied by normalization of the aortic isthmus diameter and resolution of the previously noted flow turbulence. The systolic gradient across the aortic arch decreased to less than 5 mmHg. Blood pressure differences between upper and lower limbs resolved, and femoral pulses remained strong and symmetrical. Based on these findings, the diagnosis of aortic coarctation was excluded and the initial echocardiographic features were attributed to transient ductal tissue and altered flow dynamics during physiological ductal closure. Conclusion: A ductus arteriosus in the process of closing can create a transient functional obstruction that perfectly mimics aortic coarctation, both in symptoms and Doppler measurements. Careful clinical assessment and serial echocardiography are essential to avoid misdiagnosis and unnecessary interventions.