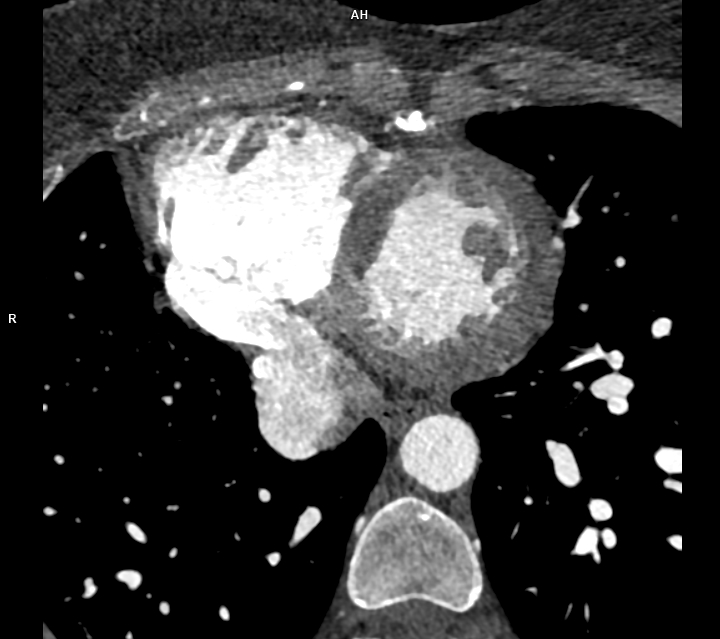
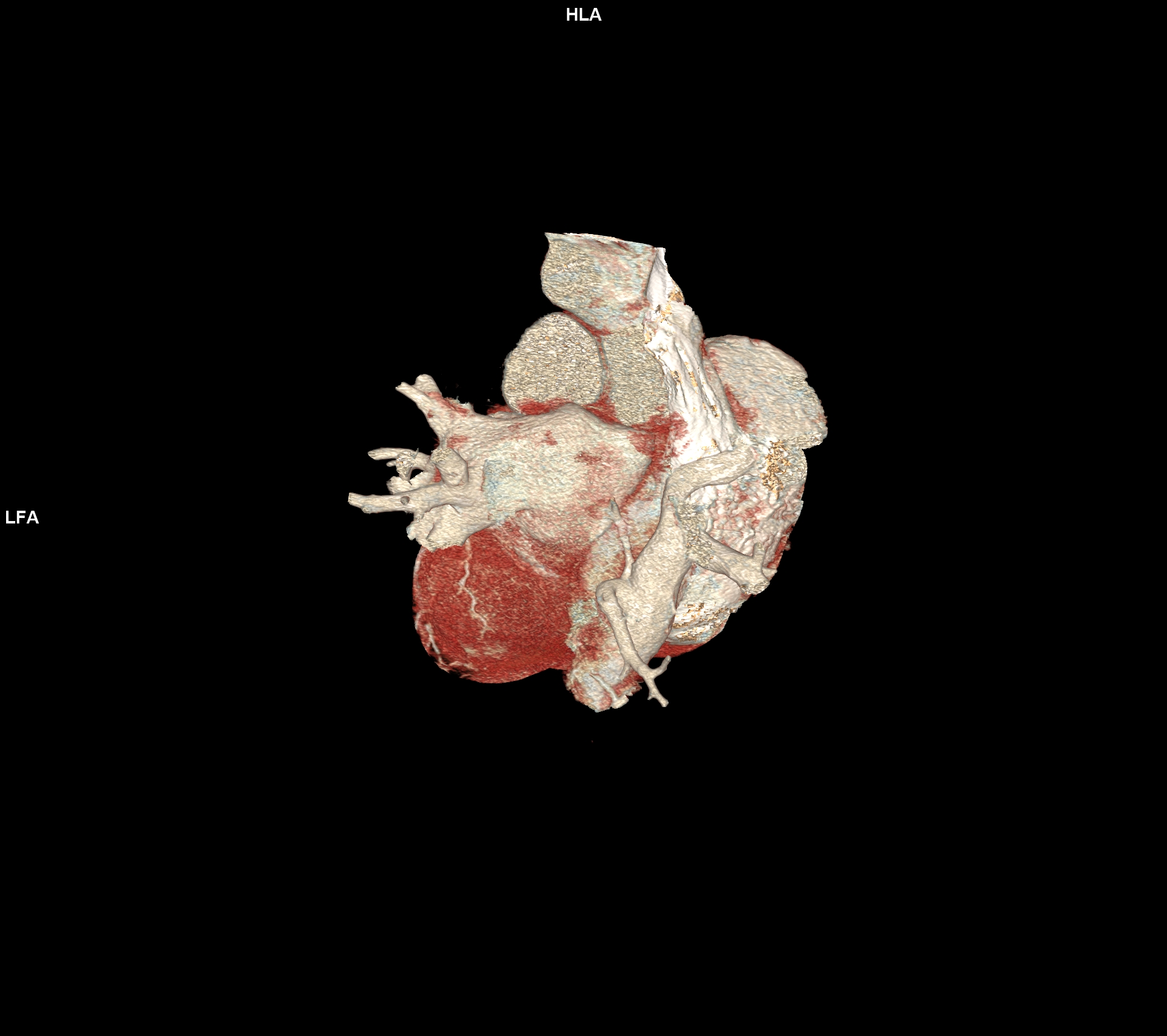
An asymptomatic 46-year-old man, with a previous childood history of Scimitarra Syndrome, underwent a high-resolution chest CT scan after a cardiological visit with normal EKG and echocardiography. No prior advanced thoracic imaging had been performed after childhood, with no more documentations of the diagnosis. Echocardiography revealed normal bi ventricular function, no chamber hypertrophy or dilation, no pulmonary hypertension, and no evidence of defects. Contrast-enhanced chest CT showed an anomalous vein draining all the right pulmonary vein into the upper limit of inferior vena cava. The characteristic inferomedial course resembled a "scimitar" on sagittal reconstruction [Fig 1]. Neither hypoplasia of the lung nor mediastinal shift were reported. No evidence of systemic arterial supply anomalies, though there was a mild enlargement of the pulmonary arteries, with evidence of a small interatrial septal defect (ASD) type ostium secundum [Fig.3, Video 1]. Scimitar syndrome presents with a broad clinical spectrum. The neonatal form is often severe, with respiratory and cardiac failure. In contrast, adult forms, such as in this case, may remain asymptomatic and are discovered incidentally. CT imaging is the gold standard for diagnosis, due to its high anatomical resolution. Although echocardiography has limitations in visualizing anomalous pulmonary venous return, it is useful for excluding associated cardiac anomalies and pulmonary hypertension. In our patient, the absence of symptoms, right chamber dilation or hemodynamic compromise, supports a conservative management strategy, with regular clinical and imaging follow-up. Conclusions. Scimitar syndrome can remain asymptomatic until adulthood and may be incidentally diagnosed through CT imaging. Almost the 50% in literature is associated to the left to right shunt, so echocardiography plays a complementary role. Surgery is the definitive treatment for scimitar syndrome. However, it is not always necessary as many patients are asymptomatic, have small left-to-right shunts, and enjoy a normal life expectancy without surgery. This case highlights the importance of thoracic imaging even in asymptomatic individuals and emphasizes the need for a multidisciplinary evaluation to determine the most appropriate management approach.