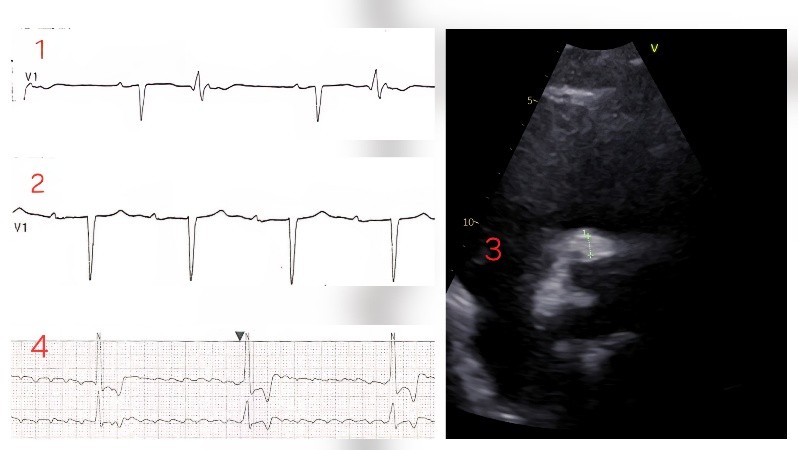
Background: Prosthetic valve endocarditis (PVE) is associated with high morbidity and mortality. Periannular extension with abscess formation is a severe complication that may result in atrioventricular (AV) conduction disturbances due to involvement of the conduction system, often requiring urgent surgical management. Case report: A 75-year-old man, who underwent bicuspid aortic valve replacement with a bioprosthesis in 2014, was admitted with progressive dyspnea, orthopnea, and peripheral edema. ECG showed sinus rhythm with PR 180 ms and ventricular bigeminism (FIG. 1). Transesophageal echocardiography (TEE) revealed thickened bioprosthetic cusps with mild regurgitation. During hospitalization, fever and decompensated heart failure developed, blood cultures grew S. Caprae and a repeat echocardiogram documented severe intraprosthetic regurgitation (PHT 300 ms, abdominal aortic flow reversal). Serial ECGs monitoring showed progressive PR prolongation (360 ms) (FIG. 2) and episodes of 2:1 AV block. Follow-up TEE demonstrated increased thickening and echogenicity of the non-coronary cusp, with perivalvular thickening and a maximum hyper-echogenic area of 8 mm involving the right coronary sinus and the mitro-aortic junction, consistent with endocarditis complicated by annular abscess formation (FIG. 3). During the following days, the patient developed bradyarrhythmic atrial fibrillation with complete AV block (HR 20 bpm) (FIG. 4), requiring temporary pacing. The conduction disorder was considered secondary to annular abscess extension. Given the rapid clinical deterioration, after having discussed the case in Heart Team, a urgent redo aortic valve replacement with annular debridement was performed. Postoperatively, sinus rhythm was restored with residual first-degree AV block without episodes of advanced conduction abnormalities. Conclusion: This case report illustrates the possible rapid progression of a prosthetic valve endocarditis complicated by annular abscess and advanced conduction disturbances. This emphasizes the need for prompt diagnosis, Heart Team evaluation, and early surgical intervention.