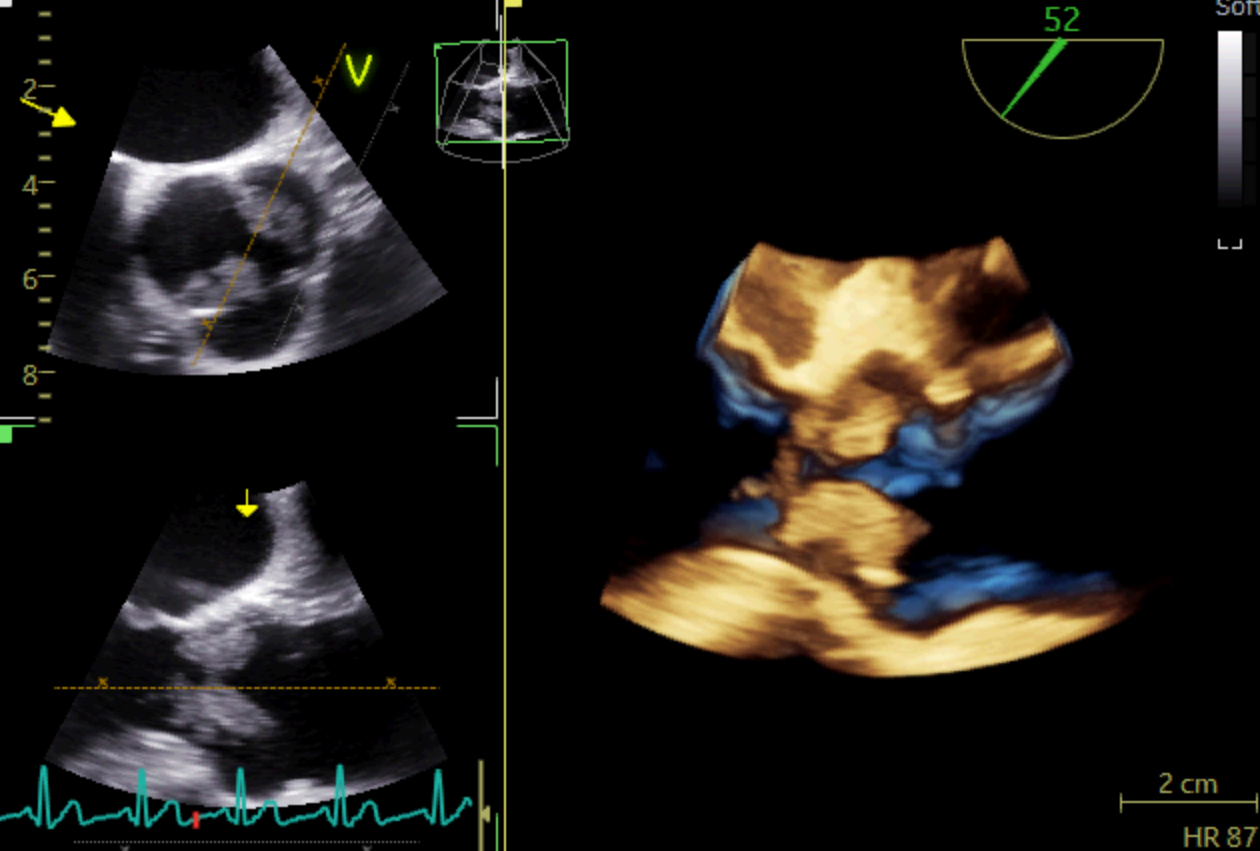
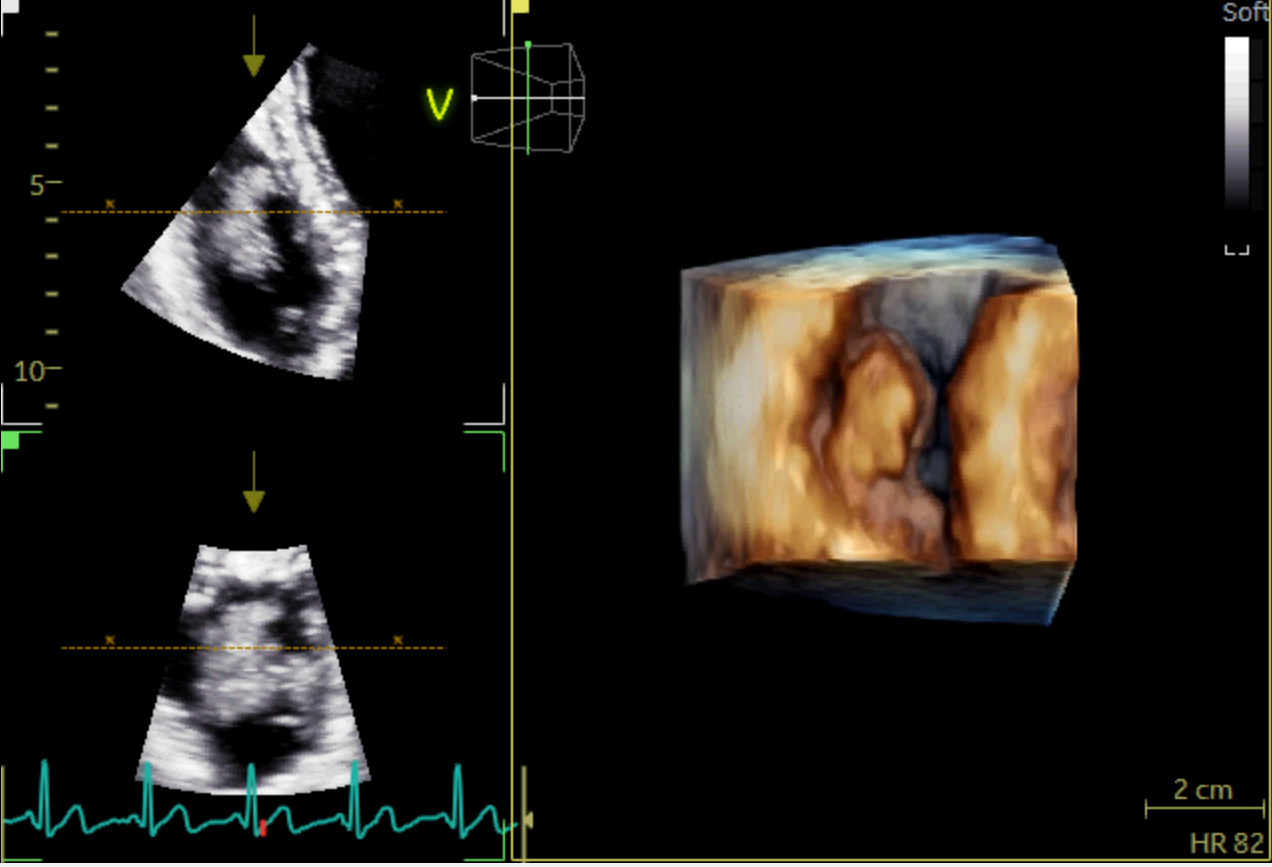
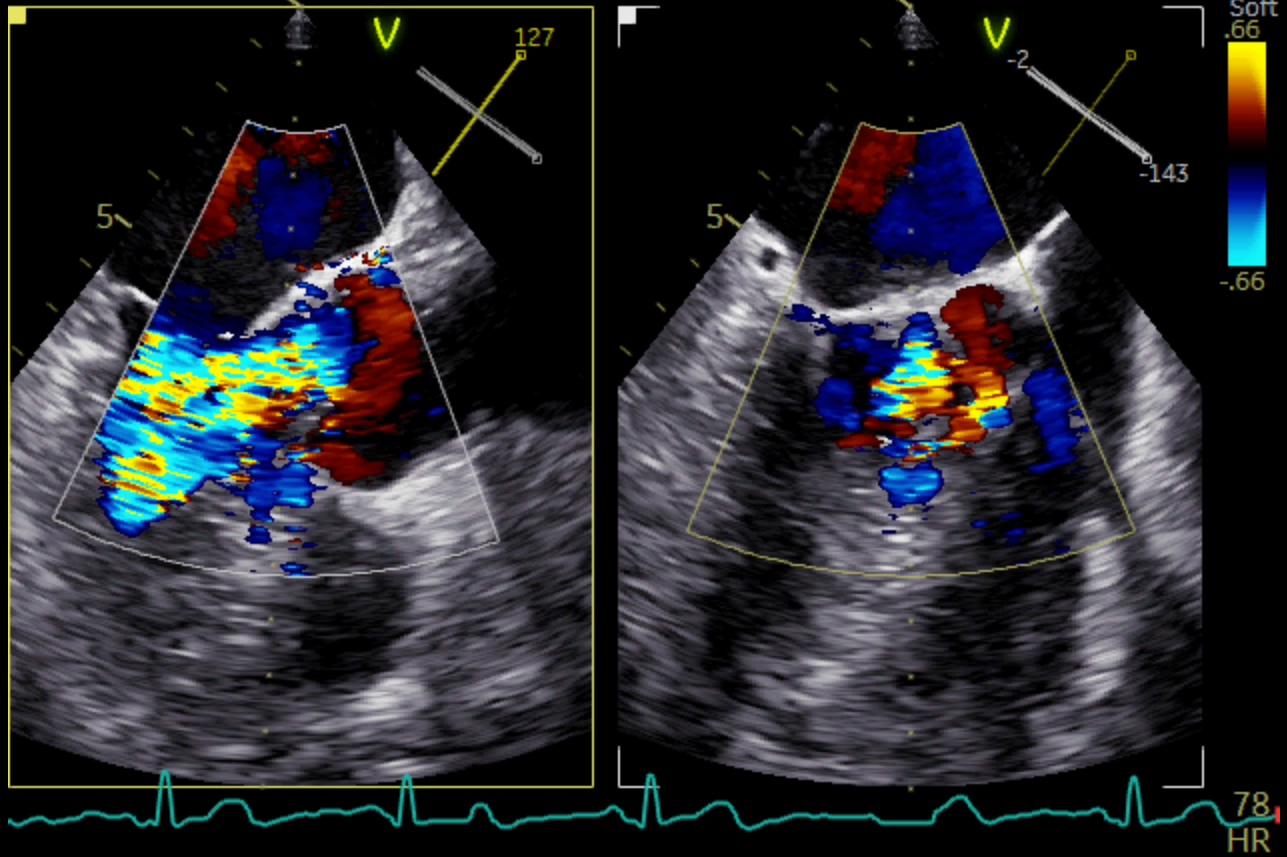
A 51 years-old man presented to the ED for dysarthria and left hemiparesis of sudden onset, dating back to approximately an hour. His past medical history included a deep venous thrombosis, currently under anticoagulant treatment, and a pancreatic cancer with hepatic metastases. Vital signs were normal and the physical examination was unremarkable except for the neurological part. The clinical suspicion of ischaemic stroke due to the occlusion of the internal left carotid artery was promptly confirmed through a CT scan and the patient successfully underwent a mechanical thrombectomy. The following day, to further investigate the nature of his thromboembolism, a TTE was performed: which surprisingly revealed two massive vegetations on the aortic and tricuspid valves. The subsequent TEE showed a circumferential three-cusp aortic involvement with a high-risk 18 mm-filamentous vegetation protruding into the left ventricular outflow tract; severe valvular insufficiency was also detected together with another large vegetation involving the subvalvular tricuspid apparatus. A total body CT-scan highlighted bilateral pulmonary embolism and splenic embolism, as further complications of the endocarditic process. During the stay the patient presented fever and blood exams were consistent with a diagnosis of sepsis; hence, upon the infectious disease specialist advice, he was started on a high-dose-ceftriaxone-and-vancomycin empirical antibiotic therapy. Eventually, blood cultures turned out negative. After a multidisciplinary meeting involving the core of the Endocarditis Team and the hospital oncologists, a conservative approach was chosen over the heart surgery, due to the patient’s critical conditions and poor prognosis. Therefore, he was transferred to the Oncology service to start palliative chemotherapy. Infective Endocarditis is frequently a difficult disease with non-specific systemic symptoms and late diagnosis; however, the onset can also be abrupt, with life-threatening complications, such as our patient’s. Multimodality imaging is key to make a prompt diagnosis of the disease and its complications and to timely plan the therapeutic strategy. A multidisciplinary management through a dedicated Endocarditis Team remains the mainstay to obtain the best clinical outcome.