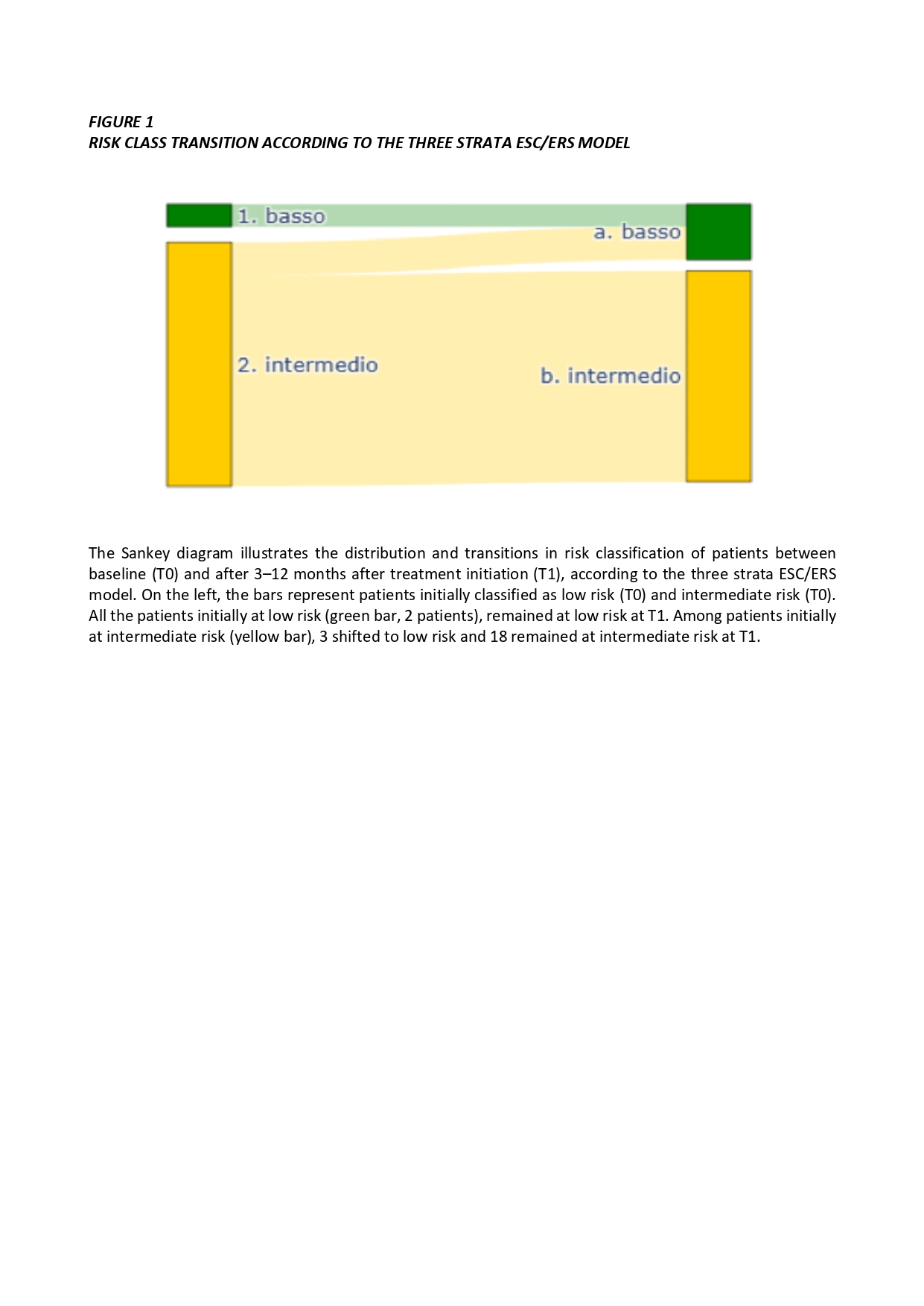
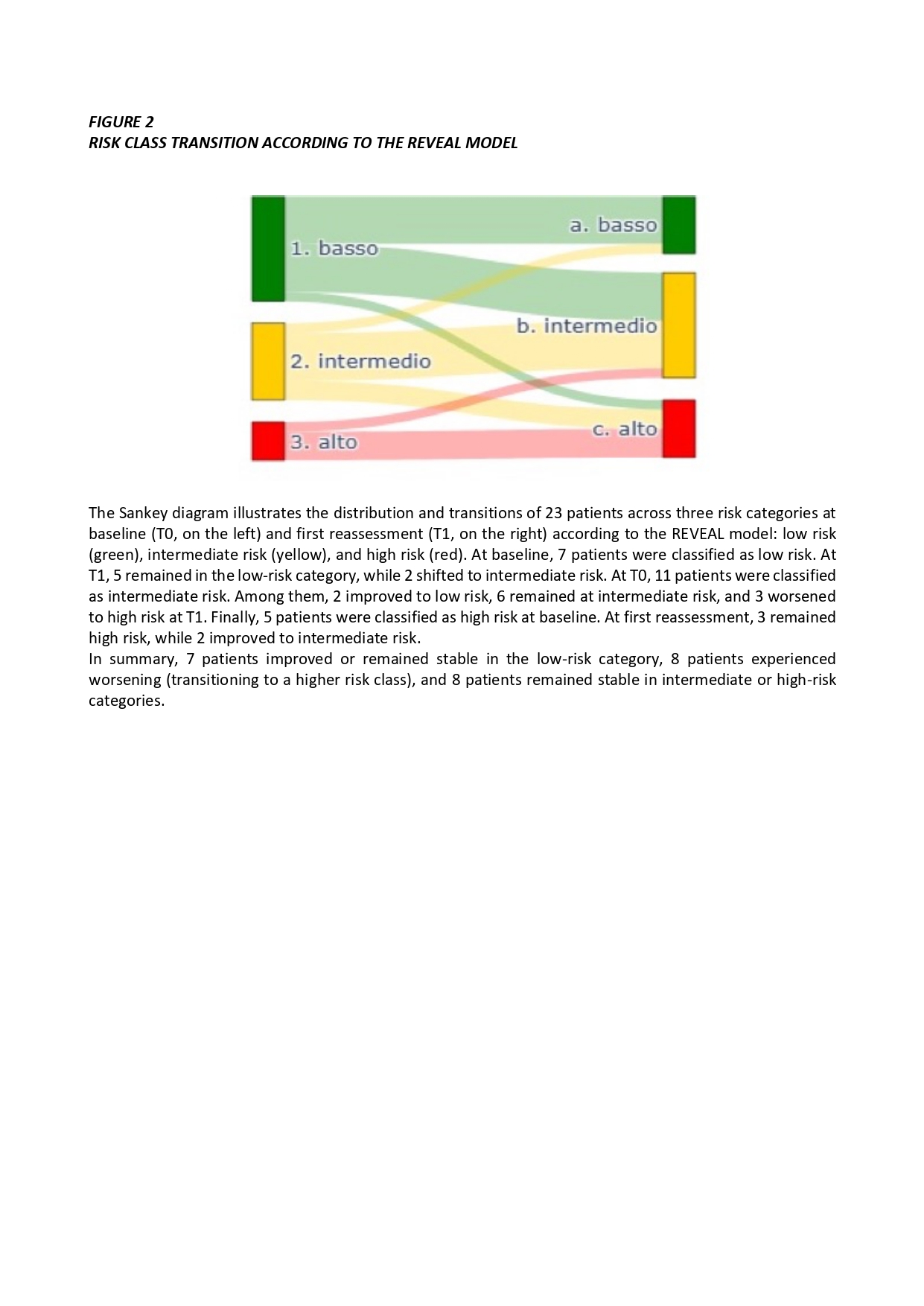
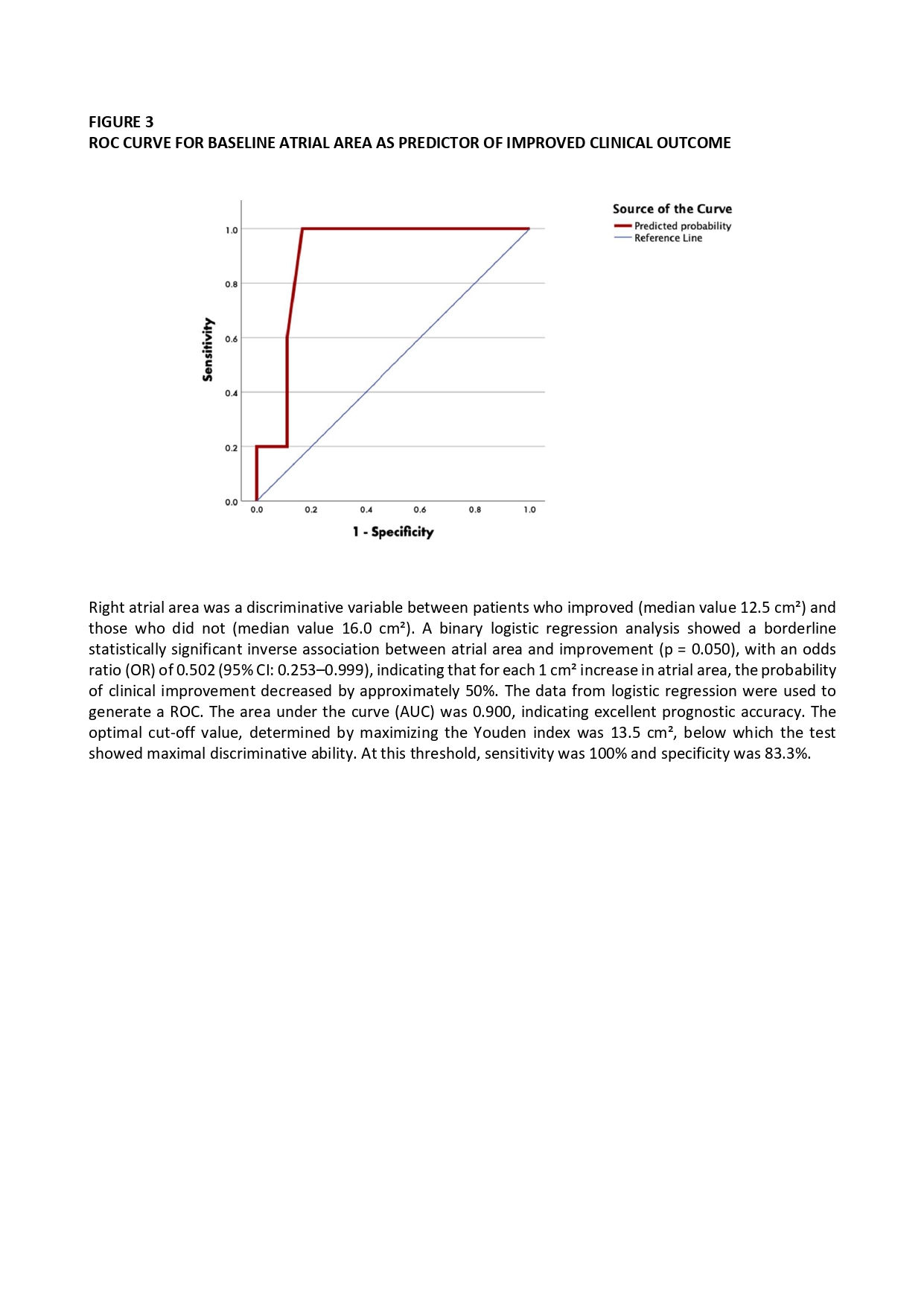
Background Systemic sclerosis–associated pulmonary arterial hypertension (SSc-PAH) is a severe complication affecting 15–18% of SSc patients, with a three-year survival rate below 50%. Early diagnosis is crucial to initiate targeted therapy. Although risk stratification tools such as the ESC/ERS 3-strata model and REVEAL 2.0 score are widely used, they were not specifically developed for SSc-PAH, potentially limiting their accuracy in this setting. Aim This study aimed to evaluate survival, therapeutic response, and prognostic accuracy of the ESC/ERS 3 strata model and REVEAL 2.0 score in patients with SSc-PAH, and to identify early predictors of clinical improvement. Methods A retrospective, observational study was conducted on 23 female patients with confirmed SSc-PAH, diagnosed by right heart catheterization and followed at a single center. Clinical, functional, and hemodynamic data were collected at baseline (T0) and after 3–12 months after treatment initiation (T1). Risk scores were applied at both time points to assess longitudinal changes and prognostic value. Results The Nine-year survival rate was 87%. Both scores showed a trend toward risk improvement after therapy although changes did not reach statistical significance (p=0.727) [Figures 1,2]. Hemodynamic parameters improved significantly, with reductions in mean pulmonary artery pressure (mPAP T0 28 mmHg* [24,5-31,0] – mPAP T1 24 mmHg [21,0-30,0]; p=0.043) and pulmonary vascular resistance (PVR T0 4,3 WU [3,4-5,9] – PVR T1 2,7 WU [1,9-2,9]; p<0.001), and an increased cardiac output (CO T0 4,6 L/min [4,1-5,2] – CO T1 5,4 L/min [4,8-6,2]; p=0.014). Functional capacity showed no substantial improvement. Baseline right atrial area (RAA) was inversely associated with clinical improvement (improved patients’ RAA T0 12,5 cm2 [10,5-13,0] – not improved patients’ RAA T0 16,0 cm2 [14,0-19,5]; OR 0.502; p<0.05), indicating early prognostic relevance [Figure 3]. Conclusions Early diagnosis and treatment are associated with improved long-term survival in SSc-PAH. However, current risk stratification models may underestimate treatment benefit in this population. Baseline right atrial area may represent a valuable prognostic marker. Development of tailored tool specifically designed for SSc-PAH is warranted to optimize therapeutic strategies. *Results are reported as median values.