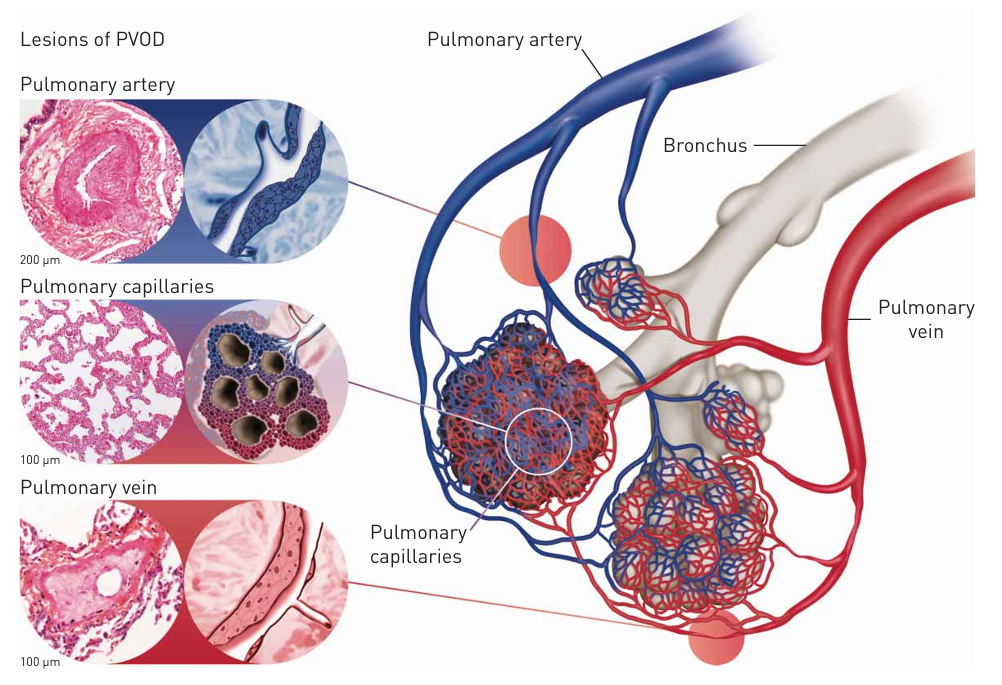
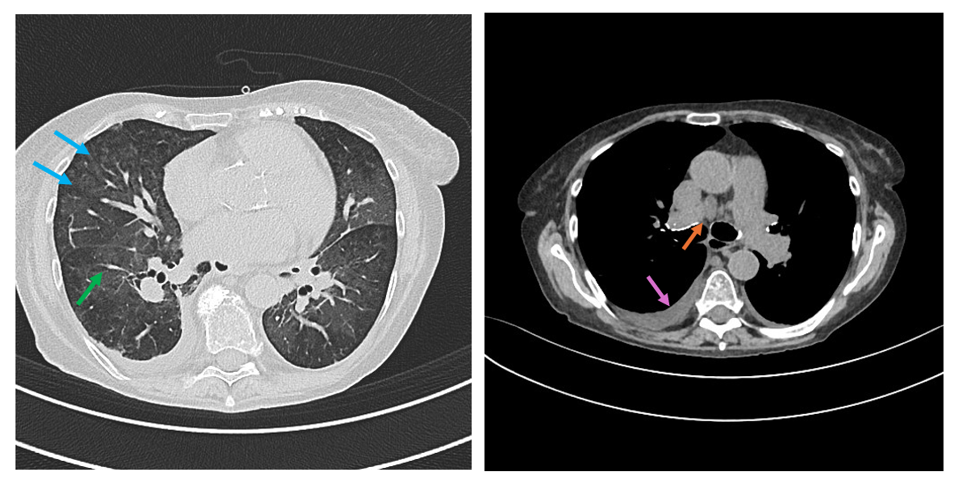
PVOD is a rare form of pulmonary arterial hypertension (PAH) characterized by remodeling of pulmonary venules with intimal fibrosis leading to lumen obliteration, progressive increase in vascular resistance, right heart failure and death. It is essential to distinguish PVOD from other causes of PAH due to its more aggressive progression, poorer prognosis and poor response to specific PAH therapies which may cause fatal iatrogenic pulmonary edema. The development of edema following pulmonary vasodilator therapy strongly supports the diagnosis of PVOD. In PVOD obstruction of small pulmonary veins impairs capillary drainage increasing pulmonary capillary pressure. Vasodilators raise precapillary blood flow without improving venous outflow (dam effect) rapidly boosting capillary hydrostatic pressure leading to edema. This paradoxical response is distinctive of PVOD and has major diagnostic and therapeutic implications. Histology is the diagnostic gold standard, but lung biopsy is contraindicated in significant PAH and a non-invasive diagnostic approach is often necessary. We report a 79-year-old woman with systemic sclerosis–associated PAH and suspected PVOD. From January 2025 the patient developed progressive exertional dyspnea and fatigue. HRCT showed centrilobular ground-glass opacities, mediastinal lymphadenopathy, smooth interlobular septal thickening and pulmonary artery dilation-features suggestive of PVOD. Pulmonary function tests revealed significantly reduced DLCO (26%). In October 2025 RHC revealed precapillary PAH (PAPm 37 mmHg; PAWP 10 mmHg; PVR 9,3 WU). Given the HRCT findings, PVOD could not be excluded, and PAH-specific therapy with macitentan was started cautiously. One week later, no heart failure signs were evident, but after 21 days the patient developed resting dyspnea with severe acute partial respiratory failure on chronic (pH 7.45; pCO2 32 mmHg; pO2 39 mmHg; sO2 72%) and was hospitalized. Imaging and clinical evaluation showed congestive heart failure likely linked to macitentan-induced pulmonary edema, which resolved rapidly after discontinuation of macitentan and a few days of oxygen therapy and iv diuretics, confirming the suspicion of PVOD. This case highlights the diagnostic and therapeutic difficulties of PVOD, emphasising the need for high clinical suspicion and extreme caution when initiating treatments targeted at PAH with very close follow-up due to the risk of rapid deterioration even several days after the start of therapy.