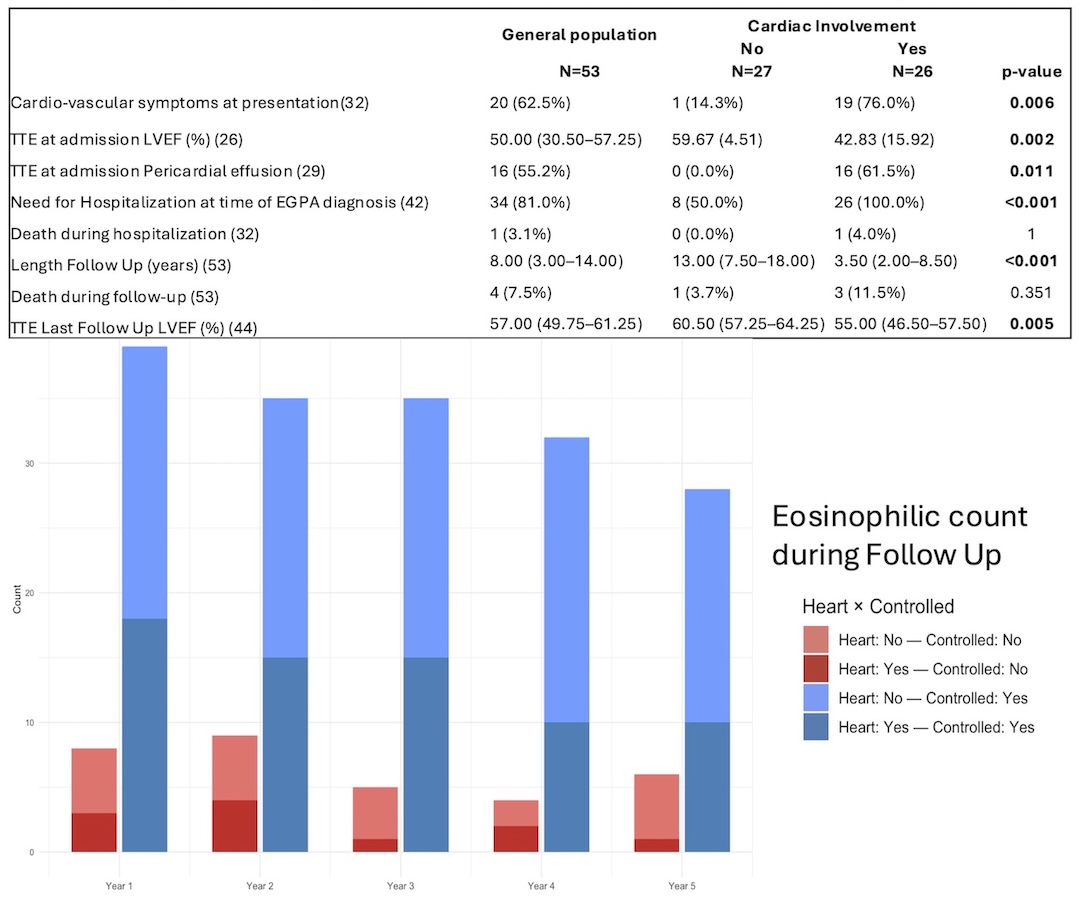
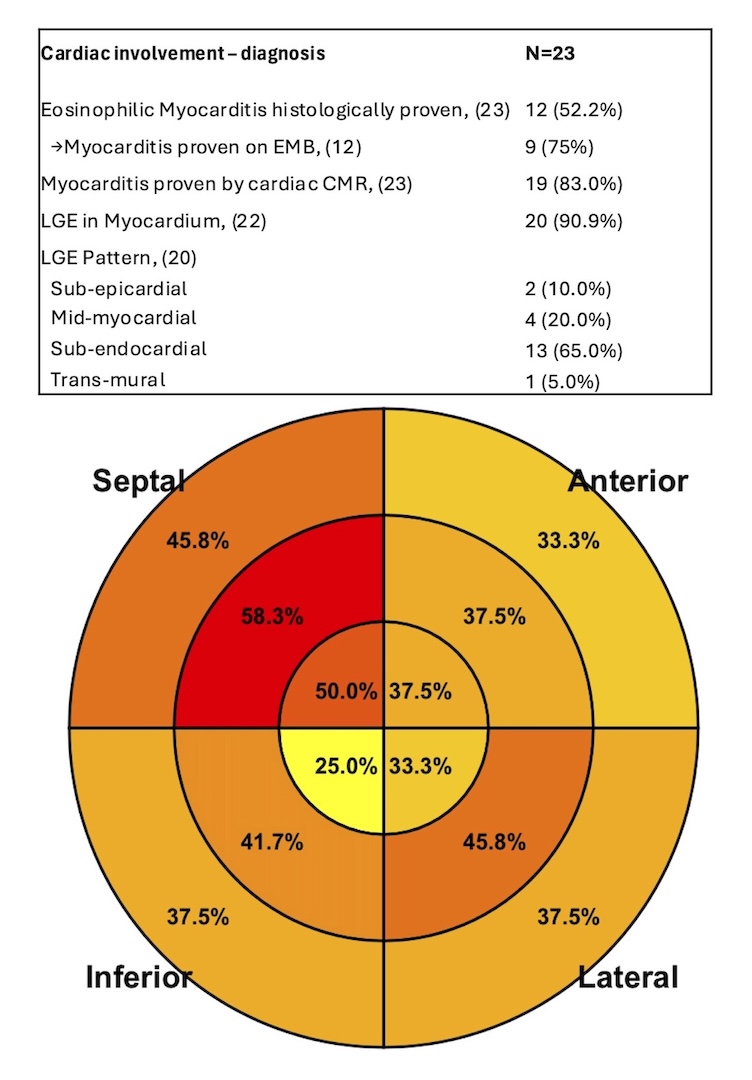
Background: Eosinophilic granulomatosis with polyangiitis (EGPA) is a rare systemic vasculitis marked by asthma, eosinophilia, and multi-organ involvement. Cardiac involvement (CI)—from pericardial effusion to eosinophilic myocarditis—is among the most severe manifestations and strongly affects prognosis. Despite advances in diagnosis and therapy, CI features and outcomes remain incompletely defined. Purpose: To characterize CI in EGPA, compare patients with CI versus non-cardiac involvement (nCI), and assess prognostic implications in a contemporary multicenter cohort. Methods: Retrospective bicenter study of 53 EGPA patients (CI n=26; nCI n=27). Baseline demographics, biomarkers, echocardiography, cardiac magnetic resonance (CMR), and endomyocardial biopsy (EMB, when available) were analyzed. Groups were compared using standard statistical tests. Results: At diagnosis, mean age was 50.5±15.7 years; 45.3% were male, with balanced traditional cardiovascular risk factors. Figure 1 displays main results of the study. CI patients had higher hospitalization rates at diagnosis (p<0.01), mainly due to cardiac symptoms. CI showed greater severity, with lower LVEF (42.8±15.9% vs 59.7±4.5%; p=0.002) and more frequent pericardial effusion (61.5% vs 0%; p=0.011). Severe presentations were common: complicated course (91.7%), cardiogenic shock (24%), fulminant myocarditis (28%), and temporary mechanical circulatory support (15.4%). Troponin and NT-proBNP were markedly elevated. At discharge, only 45.8% recovered LVEF ≥50%. Eosinophil counts and CRP did not differ between groups. ANCA-positive patients were less often male and less likely to present with CI. EMB (performed in 52.2% of CI) showed eosinophilic myocarditis in 76%. CMR confirmed myocarditis in 83%, with frequent late gadolinium enhancement (90.9%), mainly subendocardial (Figure 2), and intracavitary thrombi in 27.3%. Follow-up was longer in nCI (Figure 1). At last follow-up, LVEF remained lower in CI, while mortality was low and not significantly different between groups. Conclusions: CI in EGPA represents a severe clinical phenotype with distinctive CMR and supportive EMB findings. Cardiac symptoms often drive initial hospitalization and diagnosis. Despite low mortality with contemporary management, residual systolic dysfunction is common, supporting routine cardiac screening and long-term follow-up, especially in symptomatic patients.