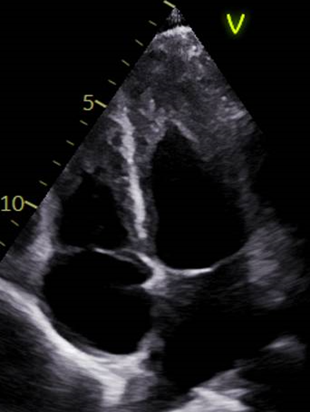
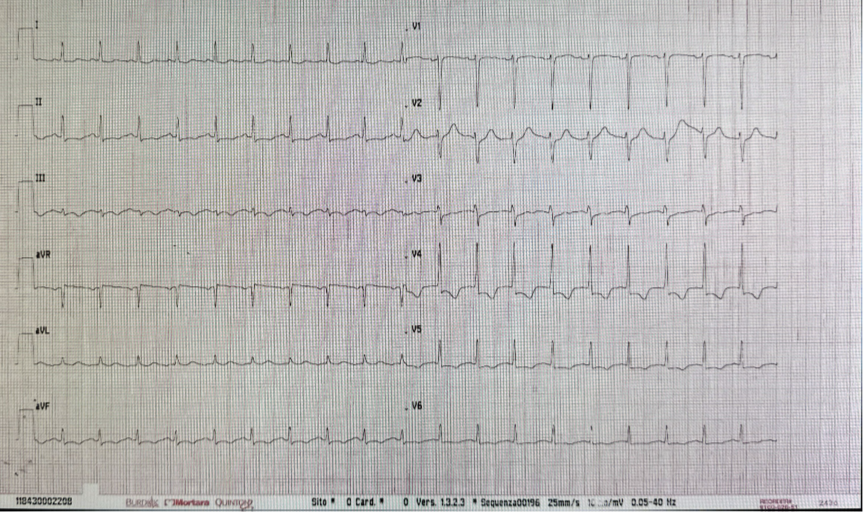
A 31-year-old man presented to the emergency department at night with chest pain at rest radiating to the left shoulder, associated with fever and abdominal pain. Symptoms had begun earlier the same day, were oppressive and constant, and partially relieved by analgesics. One month earlier, he had been diagnosed with chronic eosinophilic leukemia with PDGFRα mutation, not yet on treatment. No cardiovascular risk factors or relevant comorbidities were reported. Physical examination showed regular heart rhythm with normal heart sounds, clear lung fields, no peripheral edema, and no palpable lymphadenopathy. Splenomegaly was palpable below the left costal margin and non-tender. A maculopapular rash was present on the trunk. Vital signs revealed blood pressure 144/95 mmHg, heart rate 115 bpm, and oxygen saturation 97% on room air; the patient was afebrile. EKG (Fig. 2) demonstrated sinus tachycardia (120 bpm), short PR interval, normal intraventricular conduction, ST-segment depression up to 2 mm in anterolateral leads, and T-wave inversion in inferior leads. Laboratory tests showed leukocytosis with marked hypereosinophilia, hemoglobin 12.7 g/dL, platelet count 77,000/µL, creatinine 1.16 mg/dL, and elevated high-sensitivity troponin I (2,557 pg/mL, rising to 2,608 pg/mL). NT-proBNP was 2,009 pg/mL. Transthoracic echocardiography revealed preserved global systolic function, increased wall thickness and echogenicity in the para-apical segments with systolic obliteration of the true apex, consistent with Loeffler endocarditis (Fig.1), along with a minimal pericardial effusion and no significant valvular disease. Suspecting myocarditis, the patient was admitted to the cardiac intensive care unit. Hematology consultation led to early initiation of imatinib due to rapid clinical progression and suspected hematologic cardiac involvement. After exclusion of infectious causes, intravenous corticosteroids were administered for three days with clinical improvement. Coronary computed tomography angiography showed no epicardial coronary artery disease. Cardiac magnetic resonance demonstrated multiple non-ischemic late gadolinium enhancement areas in the mid-to-apical lateral wall and left ventricular apex, with myocardial edema, fulfilling the updated Lake Louise criteria for myocarditis (Fig.3). After complete resolution of cardiac manifestations, the patient was referred for allogeneic bone marrow transplantation and chemotherapy due to cerebral secondary involvement.