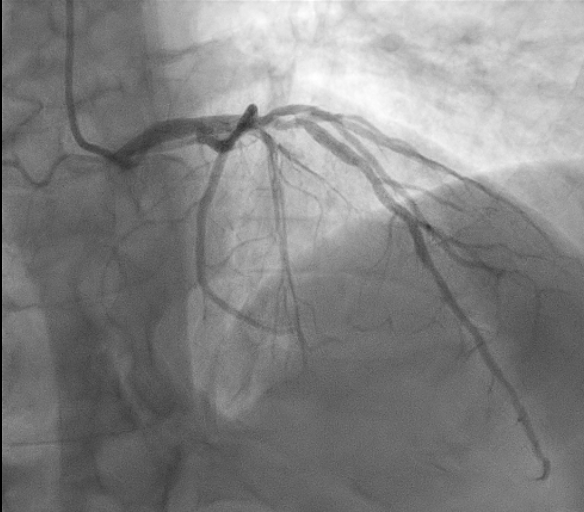
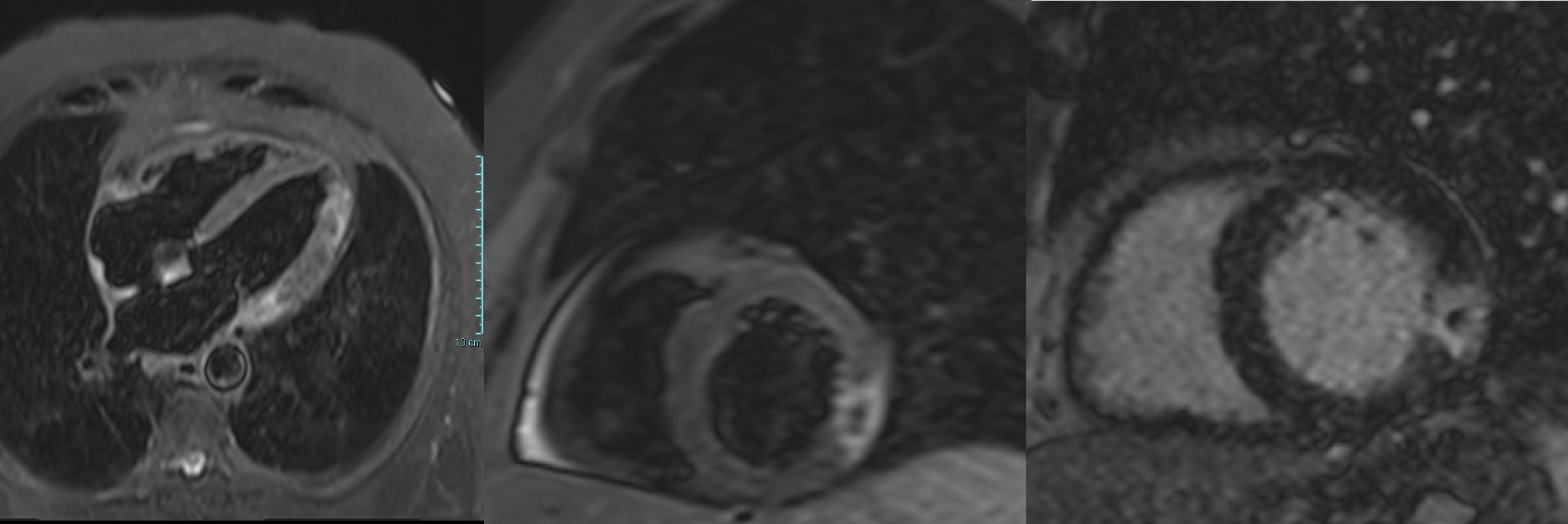
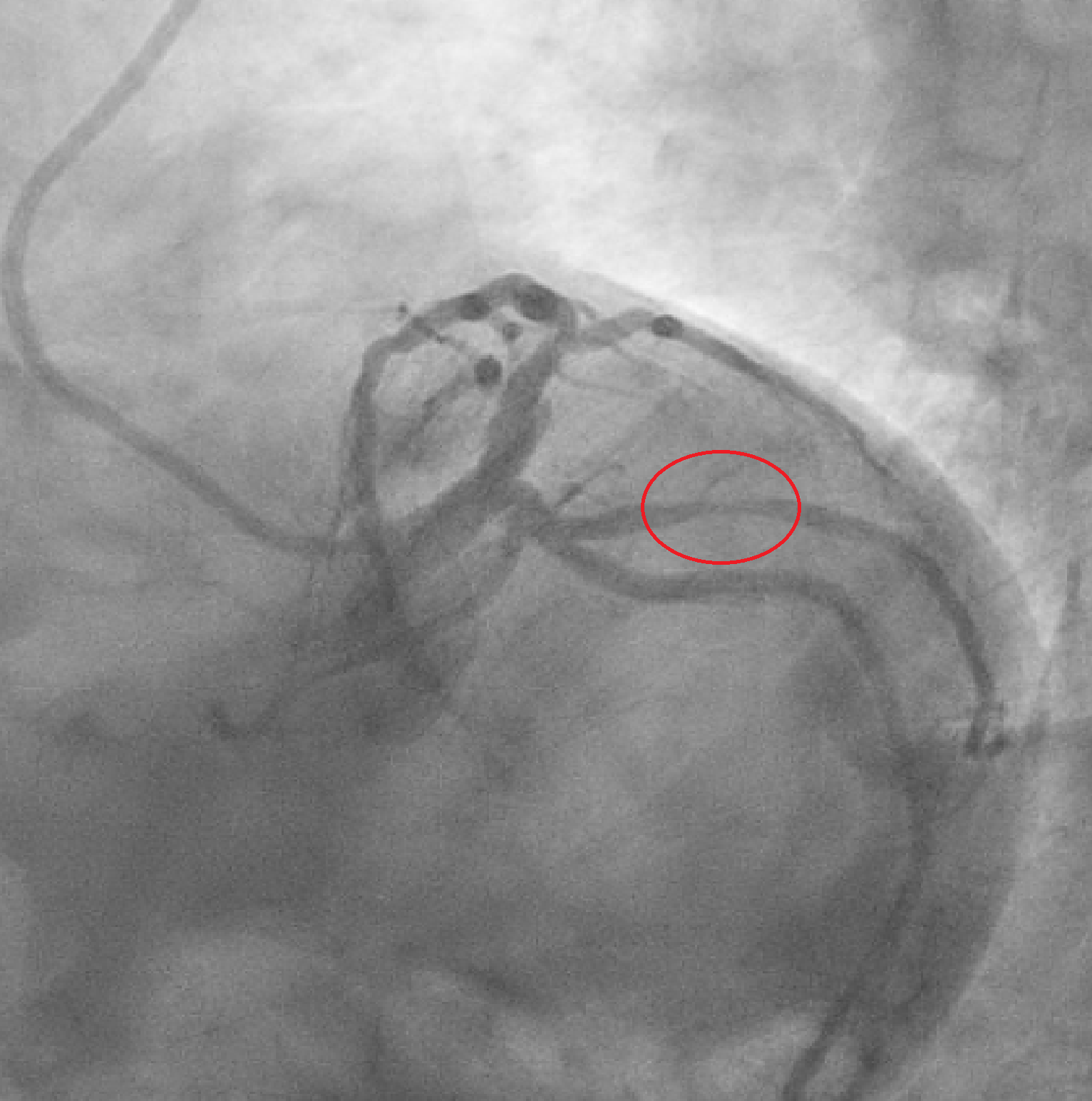
We report the case of a 65-year-old man presenting with chest pain occurring the night before. ECG showed negative T waves in the inferolateral leads. Laboratory revealed rising troponin (0.139 to 0.688 ng/mL). Transthoracic echocardiography demonstrated preserved systolic function without regional wall motion abnormalities (ejection fraction 55%). The day after, complete normalization of the ECG was observed. Patient underwent coronary angiography which revealed an intermediate stenosis of the left anterior descending artery (LAD) not functionally significant (iFR 0.91, FFR 0.87) (Fig. 1). 24-hour Holter ECG monitoring documented episodes of atrial fibrillation. He was discharged on day five with a diagnosis of myocardial infarction with non-obstructive coronary arteries (MINOCA) and referred for cardiac magnetic resonance (CMR). Discharge therapy included Aspirin, Edoxaban and Rosuvastatin/Ezetimibe. Subsequent CMR revealed myocardial edema and late gadolinium enhancement with a transmural ischemic pattern involving the basal inferolateral and anterolateral segments and the apical lateral segment and microvascular obstruction in the basal inferolateral segment, consistent with transmural myocardial infarction (Fig. 2). A subsequent review of the coronary angiogram identified an intermediate, hazy lesion in the proximal circumflex/obtuse marginal branch, compatible with the culprit lesion (Fig. 3). The patient was contacted and clopidogrel 75 mg daily was added, resulting in triple antithrombotic therapy for one month. At 30-day follow-up, the patient remained asymptomatic. This case highlights the pivotal role of CMR in clarifying the diagnosis and guiding therapy in MINOCA, even when the underlying etiology remains uncertain between coronary embolism and unstable plaque.