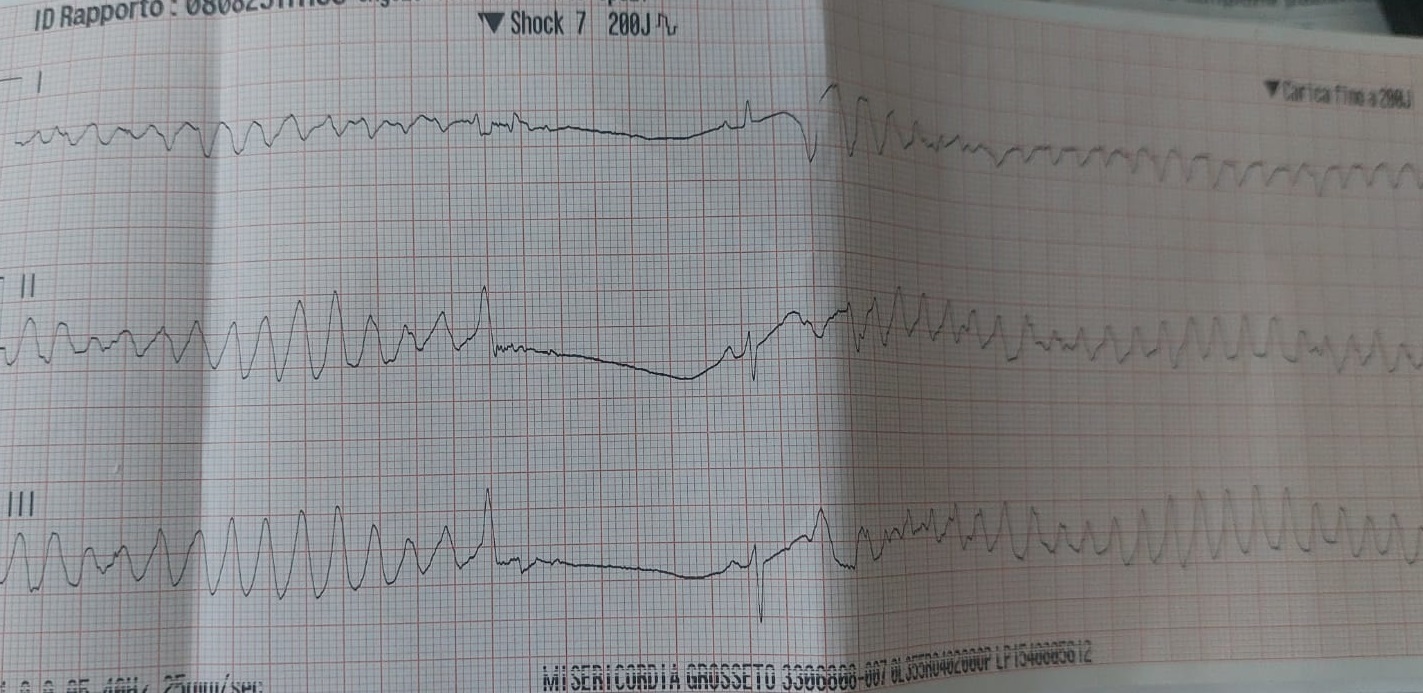
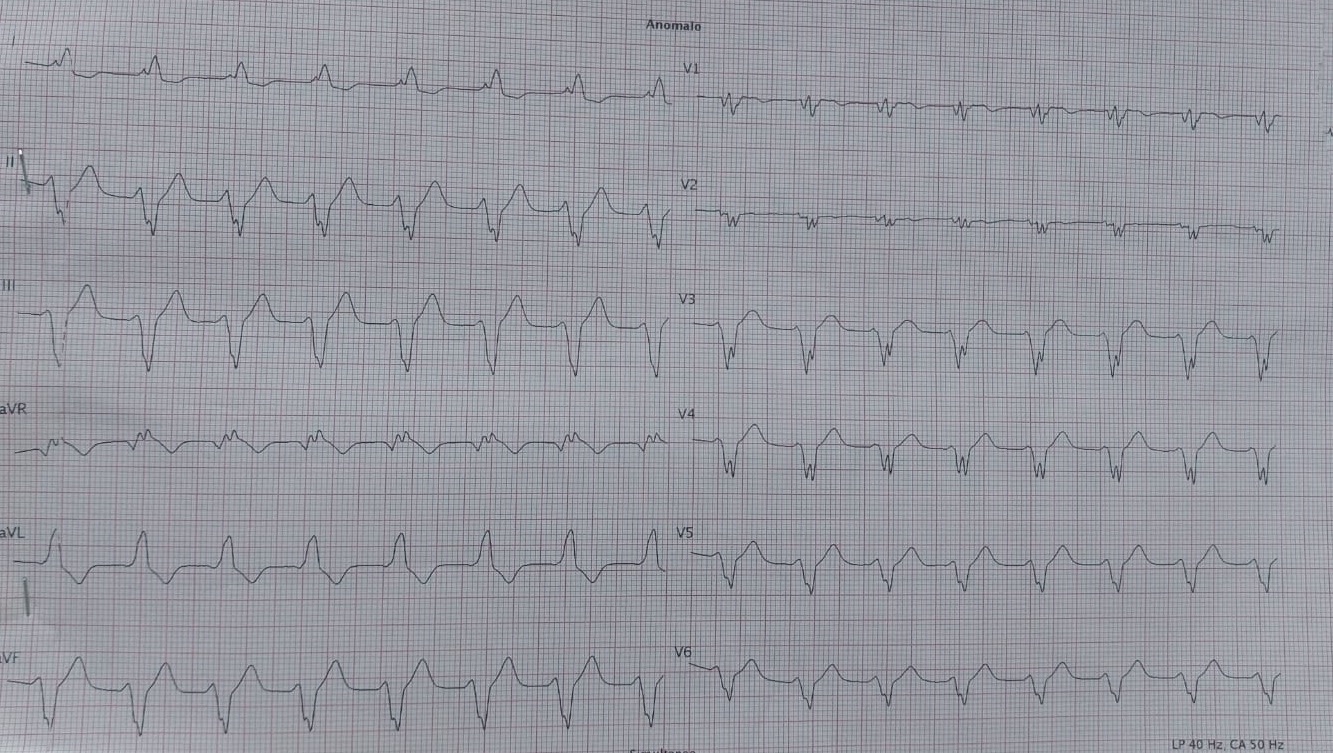
Background: Electrical storm (defined as ≥ 3episodes of sustained ventricular tachycardia or ventricular fibrillation within 24 h) is a life-threatening condition that may complicate the course of myocardial infarction, often refractory to conventional antiarrhythmic therapies. Overdrive pacing can occasionally provide effective arrhythmic suppression in selected cases, although its use as a rescue therapy remains uncommon. Case summary: A middle-aged man presented with progressive dyspnea and chest pain in subacute anterior ST-segment elevation myocardial infarction. Coronary angiography revealed proximal left anterior descending artery occlusion, successfully treated with PCI and drug-eluting stent implantation. The clinical course was complicated by acute pulmonary edema, severe left ventricular systolic dysfunction (LVEF 25%) and recurrent ventricular fibrillation consistent with electrical storm, refractory to antiarrhythmic drugs, electrolyte correction and left stellate ganglion block. The patient was trasferred to our CICU in a tertiary center, with a ccardiogenic shock condition (SCAI D) and persistent ventricular arrhythmias and worsening hemodynamics required repeated DC shocks and escalating inotropic support. A temporary transvenous pacemaker was implanted for high-rate ventricular overdrive pacing, starting at 110 bpm and increased up to 125 bpm, resulting in a marked reduction and subsequent complete suppression of VF/VT episodes. Hemodynamic stability was maintained with intra-aortic balloon pump, norepinephrine and dobutamine. The patient required continuous veno-venous hemofiltration for acute kidney injury and showed progressive neurological and ventricular function recovery. The temporary pacemaker was removed after sustained rhythm stabilization, and an implantable cardioverter-defibrillator was subsequently implanted. Conclusions: This case highlights high-rate ventricular overdrive pacing as an effective bail-out strategy for refractory electrical storm after failure of pharmacological therapy and stellate ganglion block. Suppression of triggering premature beats responsible for R-on-T–induced ventricular fibrillation was achieved. An integrated pharmacological and non-pharmacological approach was essential for managing cardiogenic shock.