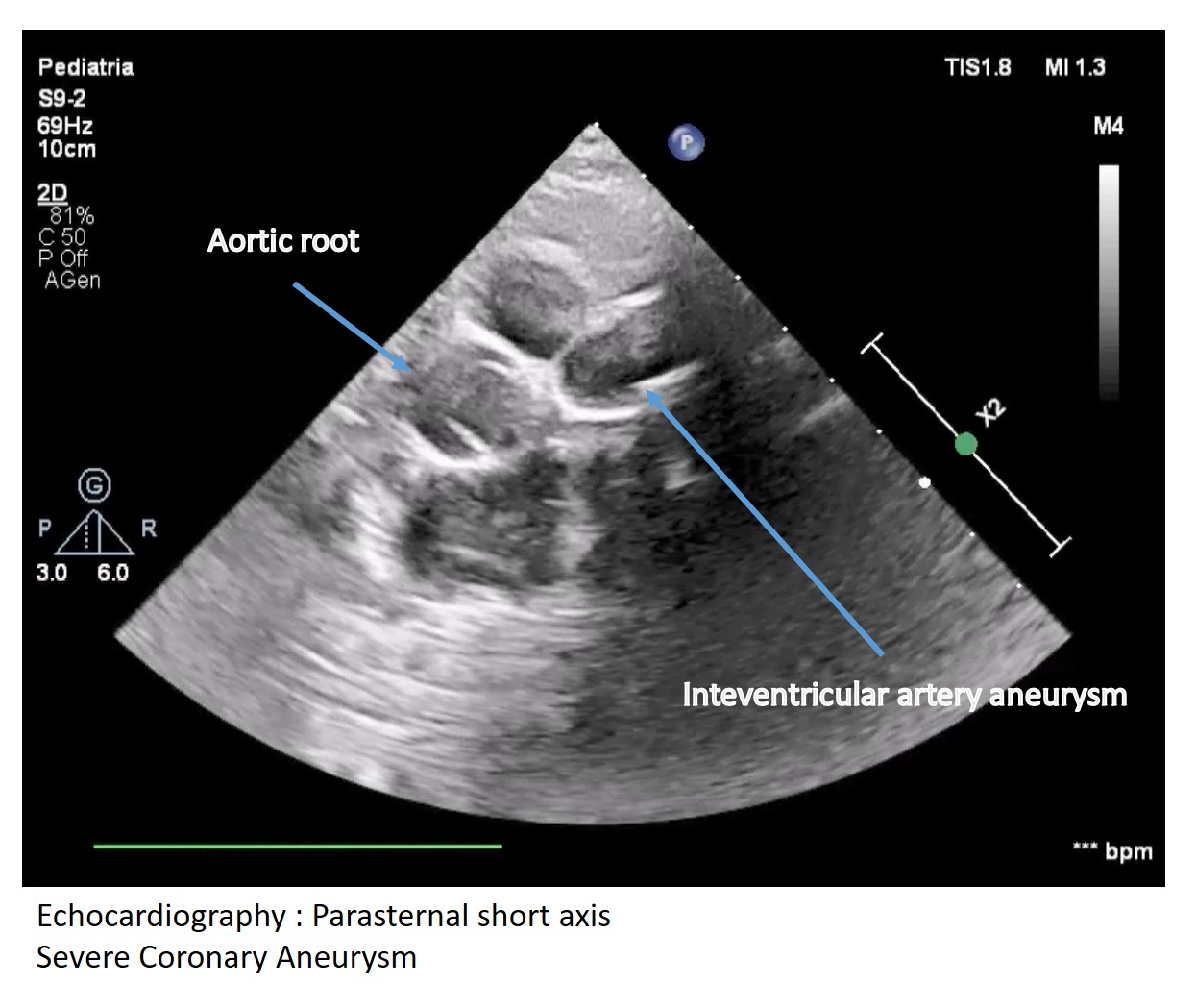
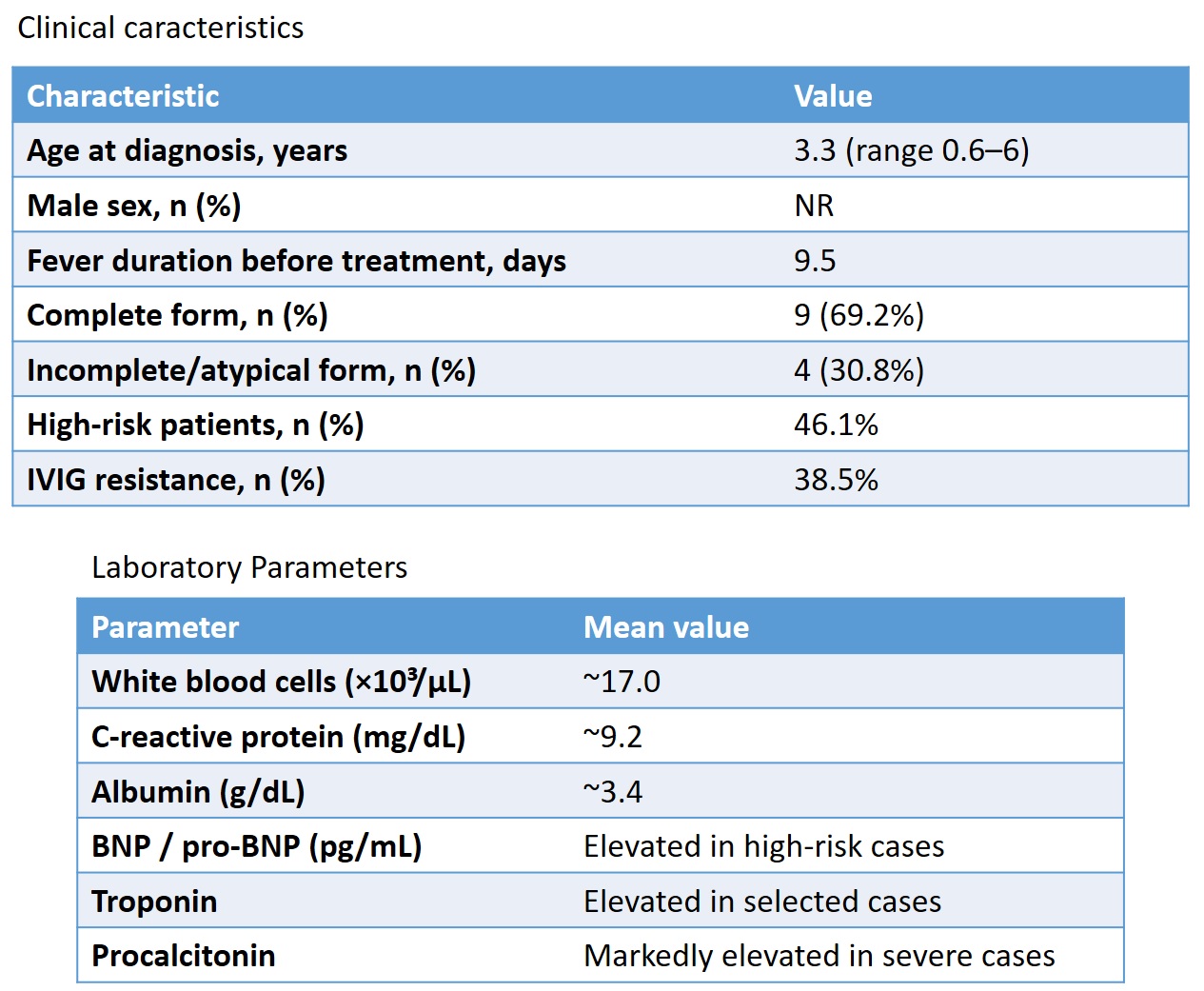
Introduction Kawasaki disease (KD) is a systemic vasculitis of childhood in which the response to intravenous immunoglobulin (IVIG) therapy represents a crucial determinant for the prevention of cardiovascular complications. A non-negligible proportion of patients shows an incomplete response or resistance to treatment, reflecting persistent vasculitic activity. Materials and Methods We conducted a monocentric retrospective observational study including 14 consecutive pediatric patients diagnosed with KD. Clinical, laboratory, and cardiological features at disease onset and during follow-up were analyzed. Resistance to IVIG was defined as persistence or recurrence of fever, or the development of aneurysms after the first IVIG infusion. Results The mean age at diagnosis was 3.3 years (range 7 months–6 years), with a mean duration of fever before treatment of 9.5 days. Baseline laboratory findings showed leukocytosis (~17,000/µL), elevated C-reactive protein (~9.2 mg/dL), and a tendency toward hypoalbuminemia (~3.4 g/dL). Incomplete or atypical KD was observed in 30.8% of the cohort. IVIG resistance occurred in 38.5% of patients, requiring a second IVIG infusion or steroid therapy. Among negative prognostic factors, delayed diagnosis and treatment, marked hypoalbuminemia, and elevated pro-BNP and troponin levels emerged as relevant. Notably, in a single patient, the persistence of leukocytosis, thrombocytosis, and conjunctival inflammation/lip fissuring after the first IVIG cycle—despite normalization of CRP and procalcitonin levels and resolution of fever—was associated with the late development of coronary aneurysms and was interpreted as a sign of residual vasculitic activity. Conclusions In our case series, beyond established severity markers, the lack of normalization of apparently “minor” clinical and laboratory findings—such as persistent thrombocytosis and conjunctival inflammation/lip fissuring—may represent indicators of ongoing active vasculitis and incomplete response to IVIG. Careful clinical and laboratory monitoring after the first IVIG infusion may support earlier and more personalized therapeutic decisions in KD patients at high cardiovascular risk.