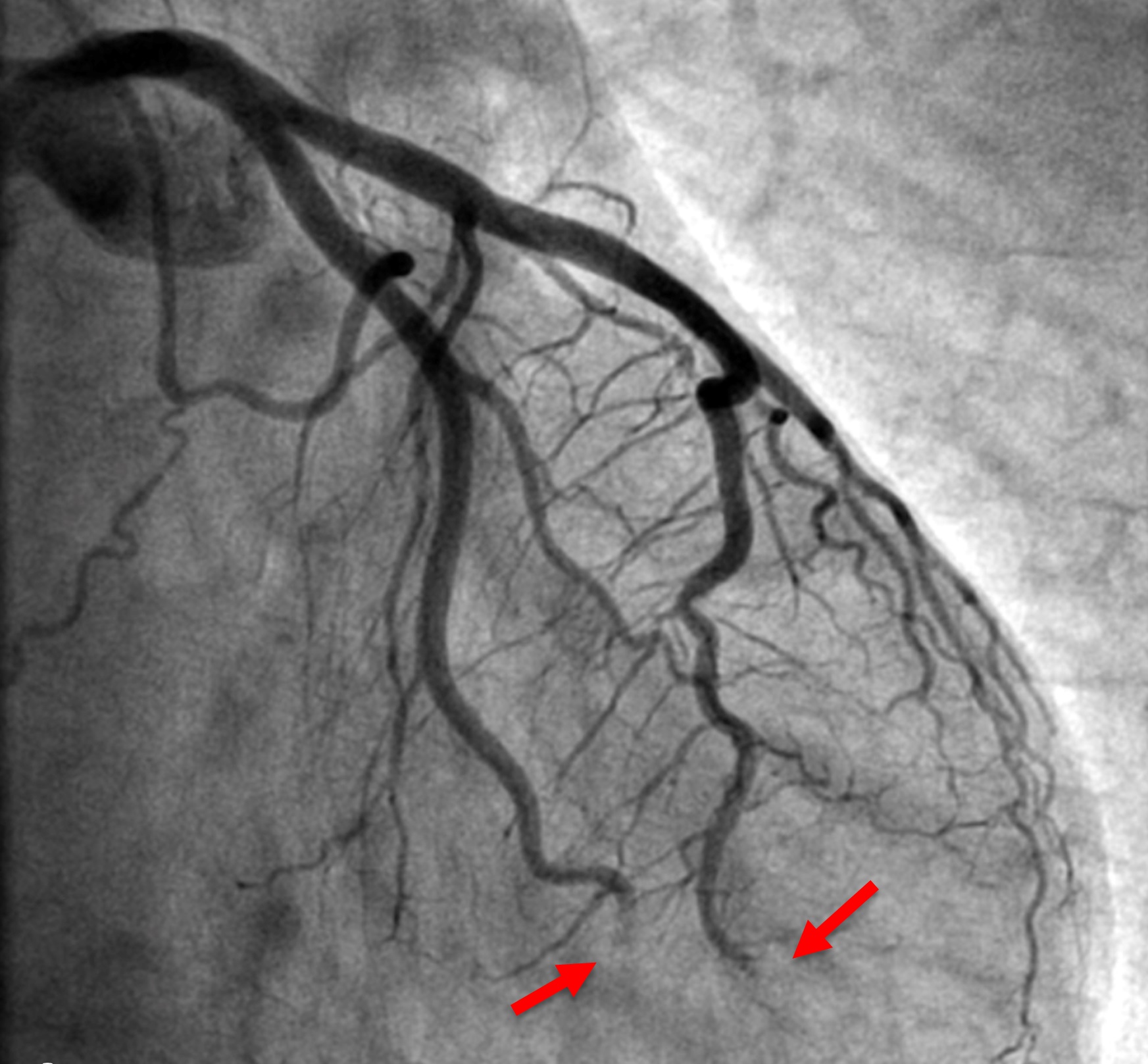
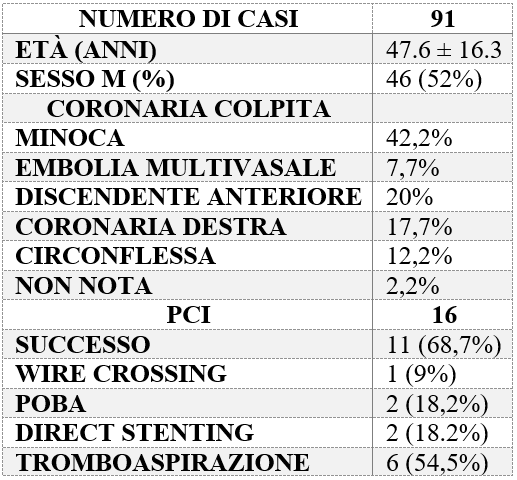
We report the case of a 44-year-old man with no risk factors presenting with chest pain after physical exertion. EKG showed ST-segment elevation in the inferior leads and atrial fibrillation. Coronary angiography revealed occlusion of the distal left anterior descending (LAD) artery and an obtuse marginal (OM) branch, suggesting coronary embolism (Fig. 1). An attempt at balloon angioplasty was ineffective. An abnormal vascular network originating from the right coronary artery (RCA) and the circumflex artery (LCX) and directed toward the left atrium was observed. Transthoracic echocardiography demonstrated a pedunculated mass measuring approximately 3 cm attached to the roof of the left atrium, confirmed by transesophageal echocardiography (Fig. 2). Further medical history revealed previous episodes of transient visual disturbance. We suspected coronary embolism due to atrial myxoma, so dual antiplatelet therapy (DAPT) was withheld to avoid delaying surgical treatment, and the patient was managed with a 24-hour infusion of tirofiban. Surgical resection was performed, and histology confirmed the diagnosis of atrial myxoma. A review of the literature shows that coronary embolism due to atrial myxoma affects men and women equally, with a mean age of 47.7 years. The most frequent presentation is myocardial infarction with non-obstructive coronary arteries (MINOCA, 42.2%). The LAD is most commonly involved (20%), followed by the RCA (17.7%) and LCX/OM (12.2%), while multivessel involvement is rare (7.7%). Percutaneous revascularization is often ineffective (successful PCI in 68.7% of cases); thrombus aspiration may aid etiological diagnosis, stent implantation may delay surgery due to the need for DAPT (Table 1).