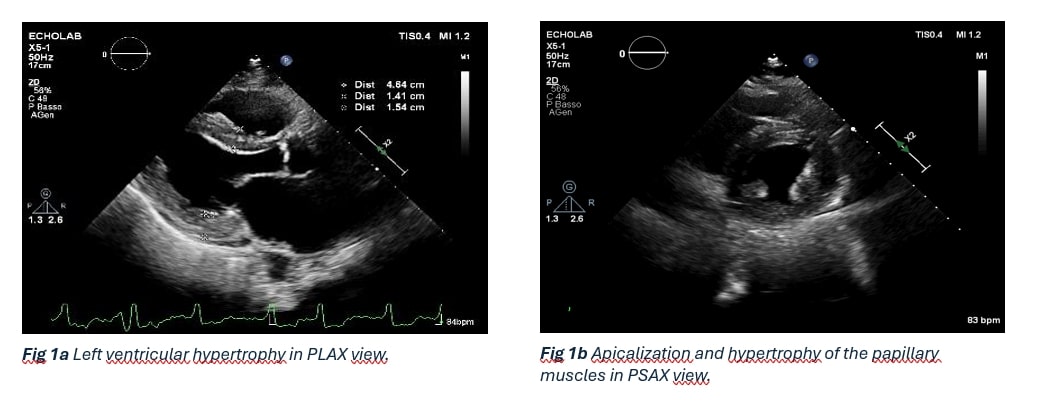
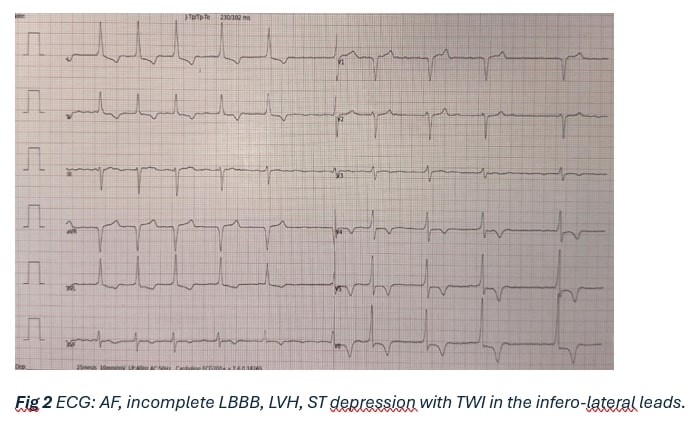
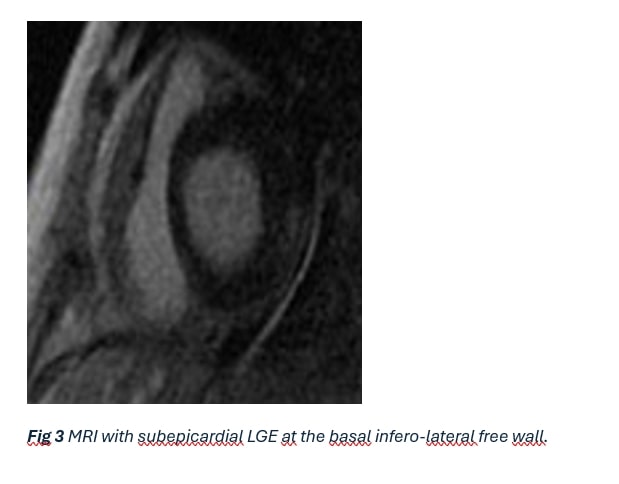
Background: A 71-year-old woman with a history of hypertension, dyslipidemia, diabetes, ischemic heart disease and permanent atrial fibrillation (since 2013) was admitted for post-infectious gonarthritis. A recent evaluation had suggested a hypertrophic phenotype, raising suspicion of infiltrative cardiomyopathy. Case Presentation: During hospitalization, a cardiological consultation was requested. The echocardiogram showed a non-dilated left ventricle with wall hypertrophy (IVS 14 mm, LVPW 14–15 mm), apicalization and hypertrophy of the papillary muscles, and a severely dilated left atrium (53 ml/m²). Systolic function was preserved (EF 62%). No systolic anterior motion (SAM), dynamic gradients, or significant valvular diseases were noted. The echocardiographic findings (Fig. 1), combined with ECG changes (incomplete LBBB, LVH, and ST depression with T-wave inversion in infero-lateral leads, Fig. 2), were more consistent with a Hypertrophic Cardiomyopathy (HCM) phenotype than an infiltrative pattern. Given the presence of several "red flags" for Fabry Disease—including proteinuria (1 g/day, disproportionate to diabetic nephropathy), bilateral hearing loss, acroparesthesia, and a history of stroke—associated with a family history of early-onset stroke and pacemaker implantation (father), cardiac MRI and genetic testing with DBS were performed. Results: Cardiac MRI confirmed mild septal hypertrophy (13 mm) and detected subepicardial late gadolinium enhancement (LGE) at the basal inferolateral wall and low native T1 mapping values (Fig. 3). Genetic testing identified a pathogenic mutation (c.680 G>A, p.R227Q) in exon 5 of the GLA gene. Laboratory tests showed normal a-GAL A enzyme activity (as often seen in females), with increased levels of LysoGb3 and cardiac biomarkers (NTproBNP 2204 pg/ml and hs-Troponin I 0.029 ng/ml). A diagnosis of Fabry Disease with multisystemic involvement (cardiac and renal) was made. Management and Outcome: Enzyme replacement therapy (ERT) with agalsidase beta was initiated. An SGLT2 inhibitor was added to her medical treatment (canrenone, irbesartan/HCTZ, apixaban). At follow-up, the patient remains clinically stable. Conclusions: This case highlights that a definitive etiological diagnosis of Fabry disease requires integrating imaging/ECG findings with family history and extracardiac "red flags." Clinicians must systematically investigate these clues to unmask rare metabolic diseases disguised as common cardiac phenotypes.