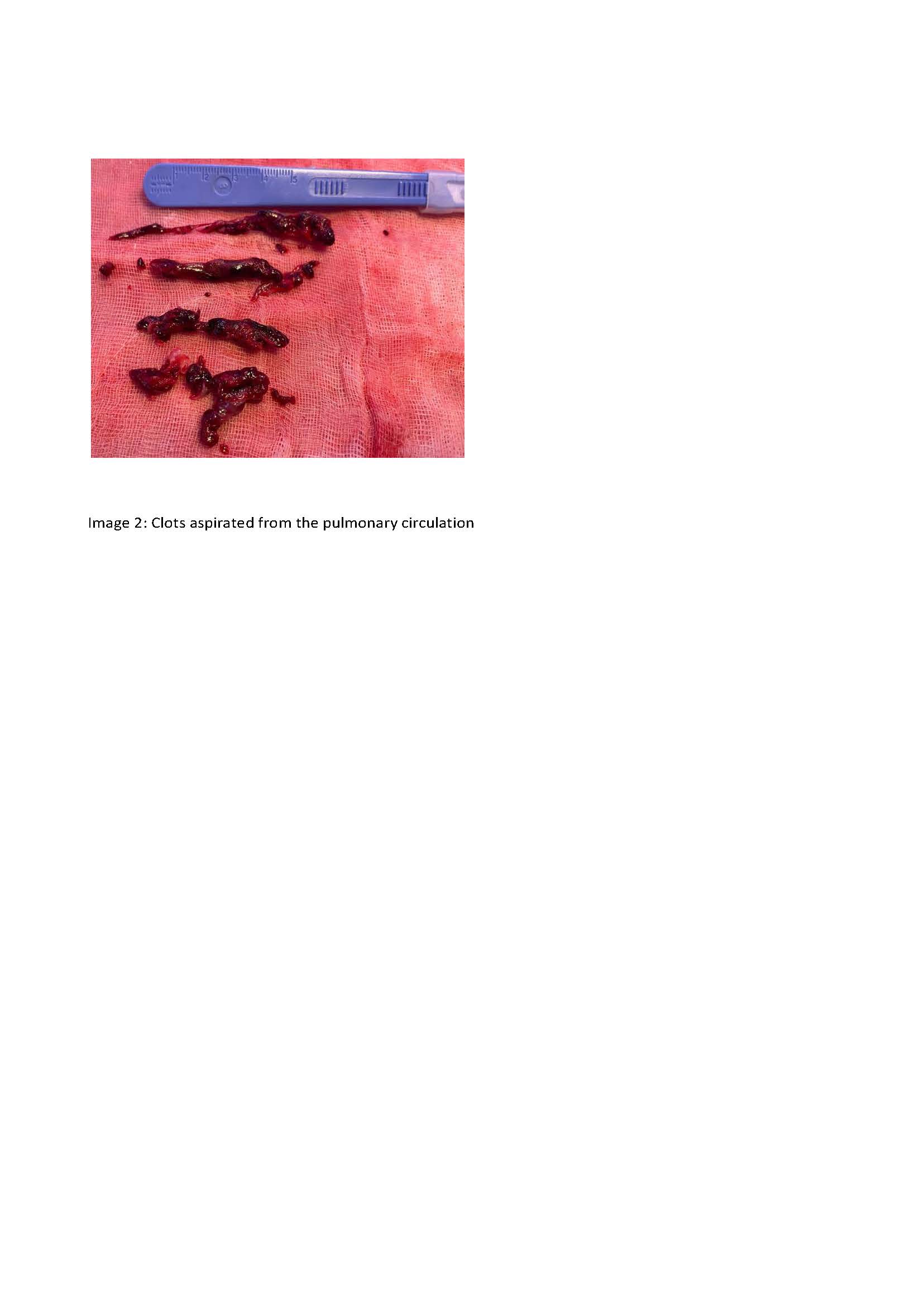
A 68 year old woman was admitted to emergency room for mental confusion. Brain computed tomography (CT) angiography revealed a giant saccular aneurysm (24 mm diameter) of the posterolateral side of the communicating segment of the right internal carotid artery and another small aneurysm of the left middle cerebral artery (image 1). The giant aneurysm was treated with percutaneous embolization, while treatment of the smaller aneurysm was deferred to a subsequent hospitalization. After a few months the smaller aneurysm was treated with the placement of 2 metal clips. On pre–discharge brain CT, subcraniotomy epidural hematoma (17 mm). After one month the patient presented hypotension and syncope. A high–risk pulmonary embolism with right ventricular dysfunction was diagnosed. Dobutamine and continuous infusion of unfractionated heparin were initiated. Due to lack of improvement, pulmonary thrombectomy was performed using FLOW TRIEVER Inari 24 F catheter (image 2). At the end of the procedure, Pulmonary Artery Pressure was 25/8 mmHg. After multiple follow–up brain CT scans and neurological assessments, anticoagulant therapy was initiated with stability on brain CT for the following 5 days. On the sixth day, the patient developed headache, confusion, and vomiting. An intra–axial hemorrhage was observed in the area adjacent to the sac of the giant saccular aneurysm, previously treated endovascularly. The aneurysm ruptured into the right lateral ventricle, resulting in tetraventricular hemorrhage. Subarachnoid hemorrhage and leftward shift of the septum pellucidum were also observed. (image 3) A new embolization procedure was then performed on the cerebral aneurysm using nine microcoils. Final angiographic control demonstrated that the cerebral aneurysm had been successfully embolized. Unfortunately, the patient did not regain consciousness. The patient was subsequently considered for organ donation with donation of the heart as well, which at pre–explant evaluation showed non–dilated right chambers and preserved systolic function. The management of pulmonary embolism in patients at high risk of bleeding remains challenging, and standardized treatment pathways are lacking. The advent of novel percutaneous devices for pulmonary embolism treatment represents an important therapeutic option.