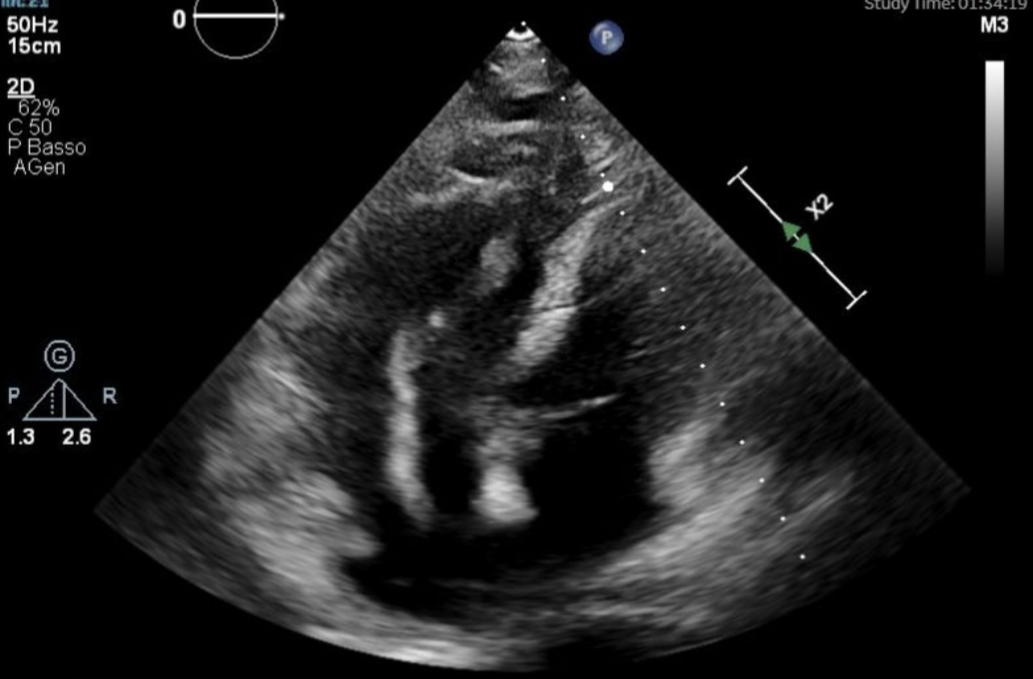
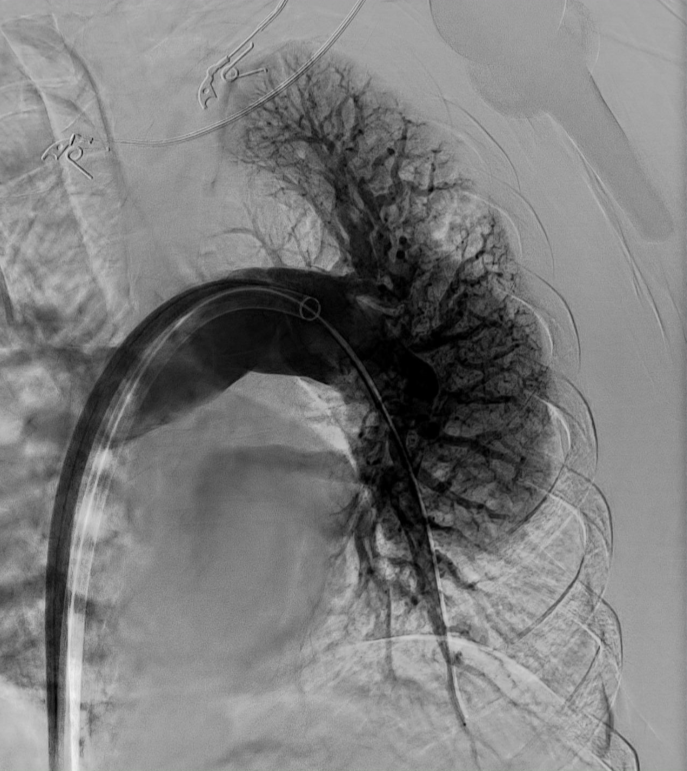
Background. A 63 yo woman with a history of arterial hypertension, atrial fibrillation and breast cancer, recently bedridden due to a depressive condition, presented to the emergency department with acute dyspnea. At admission, she was tachypneic and hypoxemic, non-invasive PA was 90/50 mmHg. ECG showed atrial fibrillation at 80 bpm with right BBB, TTE showed RV dilation and dysfunction (TAPSE 12 mm, RV S’ 9 cm/s), D-shape of interventricular septum, moderate tricuspid regurgitation (sPAP 40 mmHg) and multiple masses floating in the right sections; LV function was preserved. First suspicion was acute pulmonary embolism with initial hemodynamic compromise (pre-test probability was intermediate-high, Wells score 5.5). The patient was admitted to the ICCU. Methods. CT pulmonary angiography showed massive saddle PE with bilateral involvement and RV enlargement. Laboratory tests showed elevated D-dimer and BNP, hs-TnI 26 pg/mL. Systemic thrombolysis with alteplase was administrated, followed by iv. heparin. The patient remained dyspneic and TTE showed persistent RV dilatation and dysfunction, even though intracardiac thrombi were no longer visible. Control CT showed new triangular parenchymal consolidations, consistent with pulmonary infarction, along with worsening respiratory distress. Doppler ultrasound revealed right popliteal vein thrombosis. Diagnostic pulmonary arteriography confirmed extensive bilateral thrombi, so rescue catheter-directed mechanical thrombectomy was performed. Multiple aspiration passes with a 20 Fr Inari FlowTriever system, with blood reinfusion via the FlowSaver system, achieved significant thrombus removal and an improvement in pulmonary pressures. Results . There was a rapid improvement in clinical conditions and cardiac imaging data. The patient was discharged with oral anticoagulant therapy (edoxaban). Conclusions. Massive PE often requires systemic thrombolysis, though this may fail. Persistent clot burden increases the risk of CTEPH, associated with poor prognosis. Catheter-directed mechanical thrombectomy represents an effective and safe rescue option. Multimodality imaging and a multidisciplinary approach were key to achieve best clinical management.