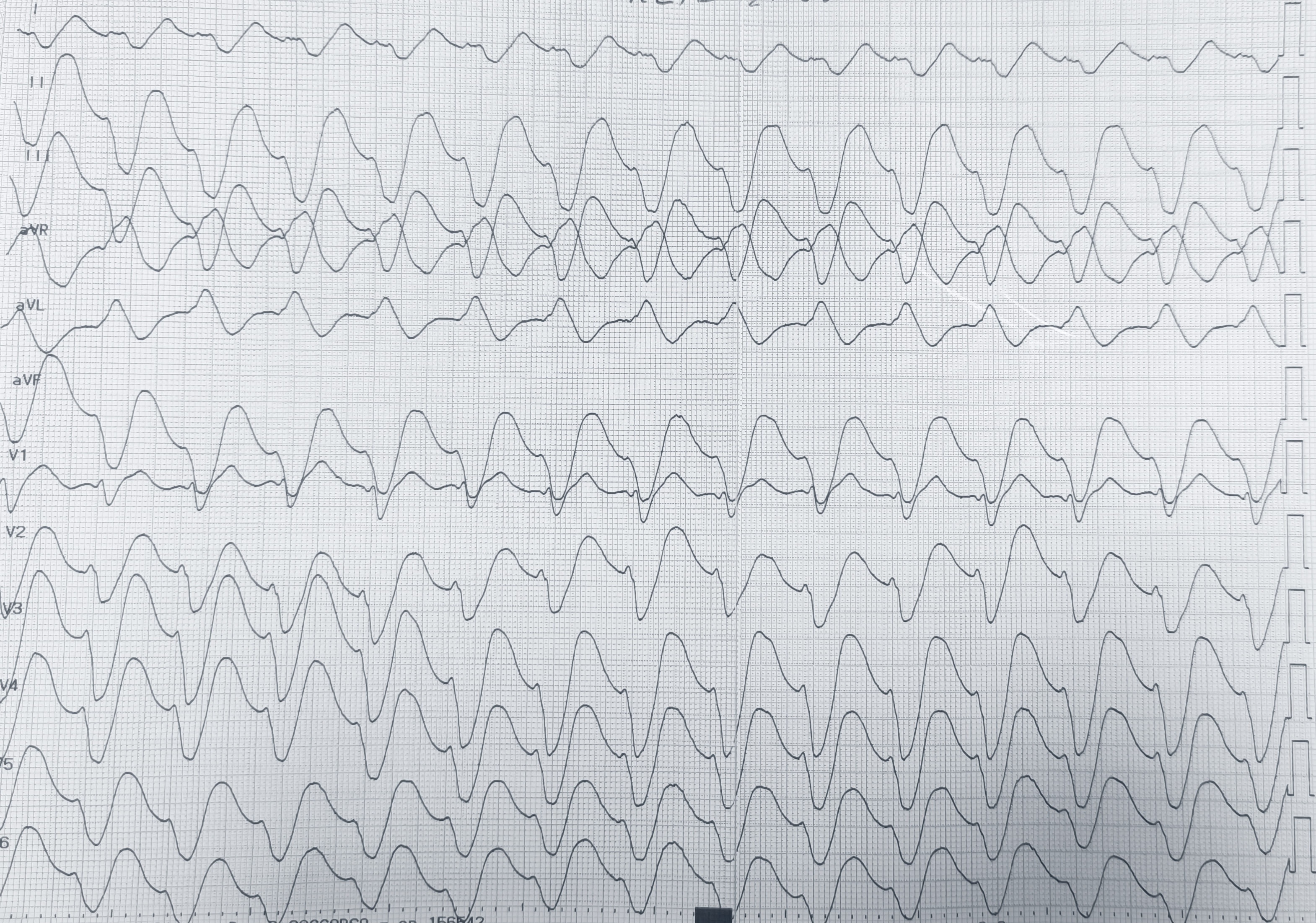
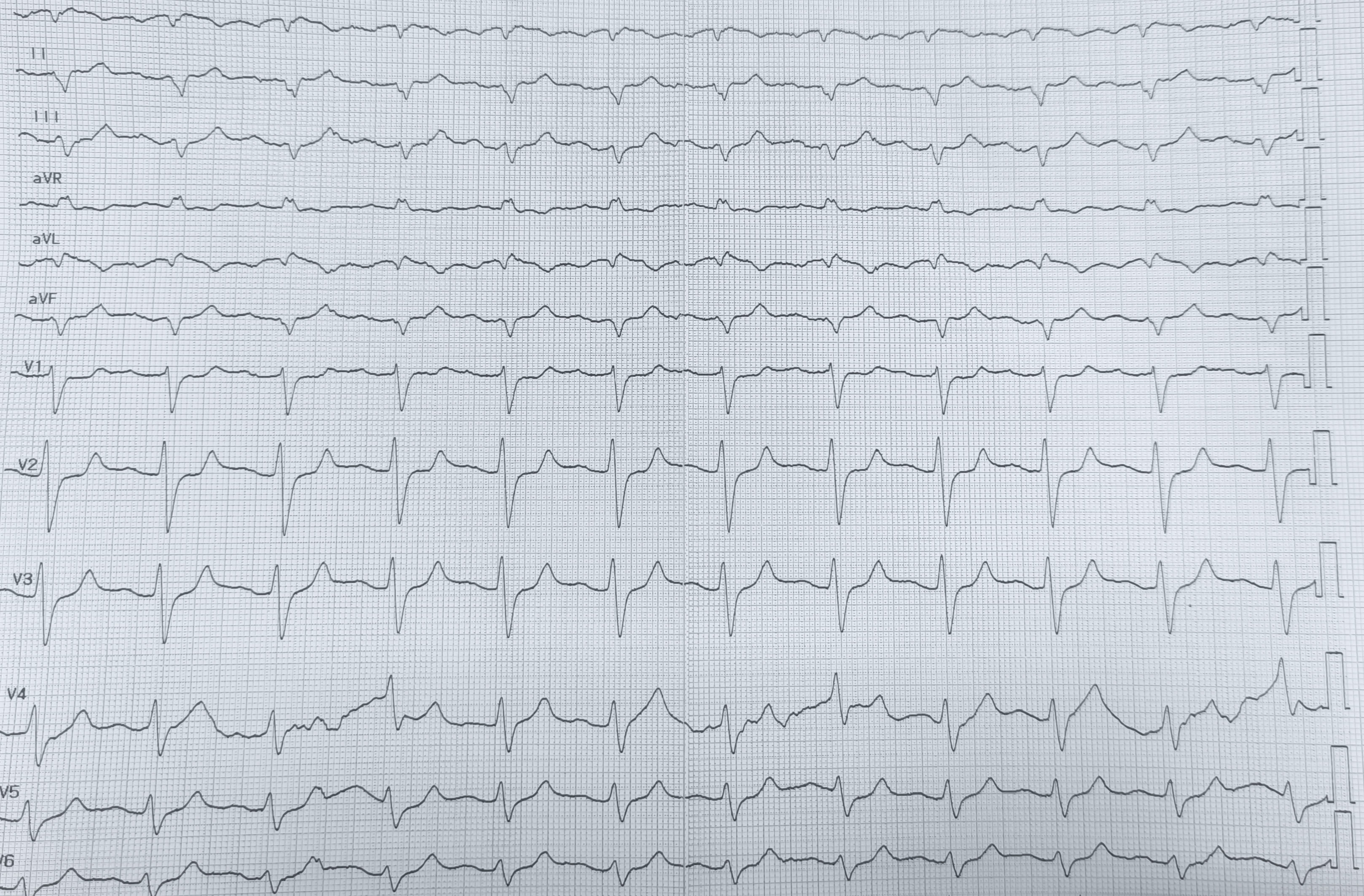
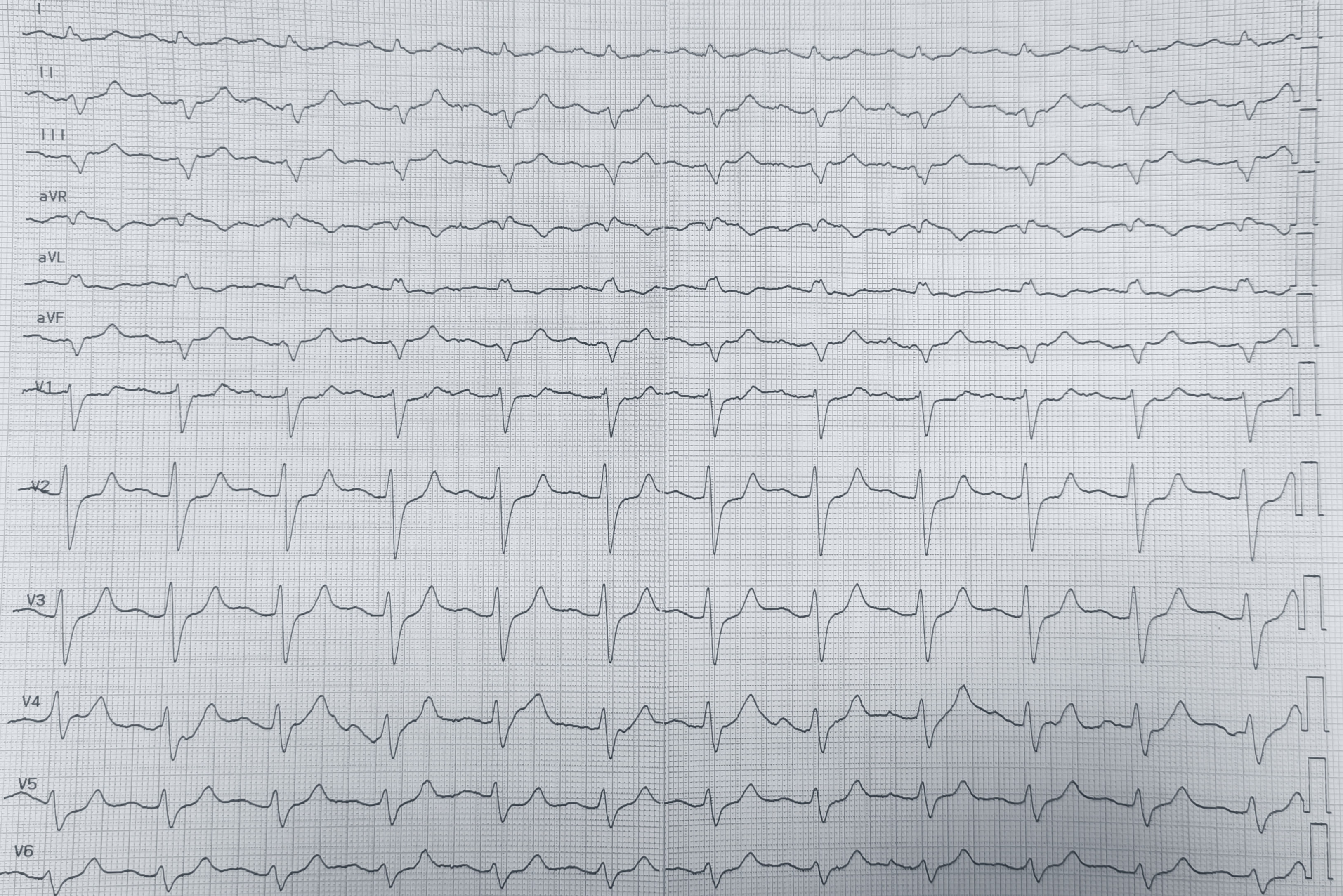
A 78-year-old patient with arterial hypertension, paroxysmal atrial fibrillation, prior ischemic stroke with post-ischemic epilepsy, active smoking, and Kartagener syndrome presented to the Emergency Department for repeated vomiting and fever; the home medication history was initially unavailable. On arrival, blood pressure was 90/60 mmHg and oxygen saturation 95%. Arterial blood gas showed pH 7.2, pCO2 49 mmHg, HCO3- 22 mmol/L, anion gap 15, lactate 2 mmol/L, sodium 137 mmol/L and potassium 5 mmol/L, consistent with mixed acidosis with dehydration. Electrocardiography with right-sided precordial leads (Fig.1) showed tachycardia with extremely wide complexes, gross repolarization abnormalities, and markedly prolonged corrected QT interval, consistent with sodium-channel blockade. Transthoracic echocardiography with dextrocardia views showed preserved biventricular function, no significant valvular disease or effusion; the inferior vena cava and internal jugular veins were small, supporting hypovolaemia. Treatment included a prokinetic agent, rapid intravenous fluids, magnesium sulfate 2 g bolus, and sodium bicarbonate 160 mEq bolus followed by 8.4% infusion. Within ~10 minutes, clinical status and the electrocardiogram improved. A control tracing was misleading due to incorrect limb-lead placement, producing an apparent extreme right axis (Fig.2); repeat with correct limb-lead inversion (Fig.3) showed sinus rhythm with first-degree atrioventricular delay, moderately widened QRS with a left bundle-branch block–like pattern, and corrected QT interval near the upper normal limit, without primary ST-T abnormalities. The caregiver later confirmed chronic flecainide 50 mg and lacosamide (a sodium channel–blocking antiepileptic drug). Laboratory tests revealed acute kidney injury with normal electrolytes. We diagnosed combined flecainide and lacosamide accumulation precipitated by vomiting-related dehydration, acidosis, and acute kidney injury. Prompt recognition of the wide-complex toxicity pattern enabled targeted therapy despite uncertain history; correct lead placement and modified imaging in dextrocardia were essential to avoid time-critical misinterpretation. This highlights that sodium-channel–blocking drug toxicity may be severe even at therapeutic doses when dehydration, acidosis, and renal dysfunction coexist.