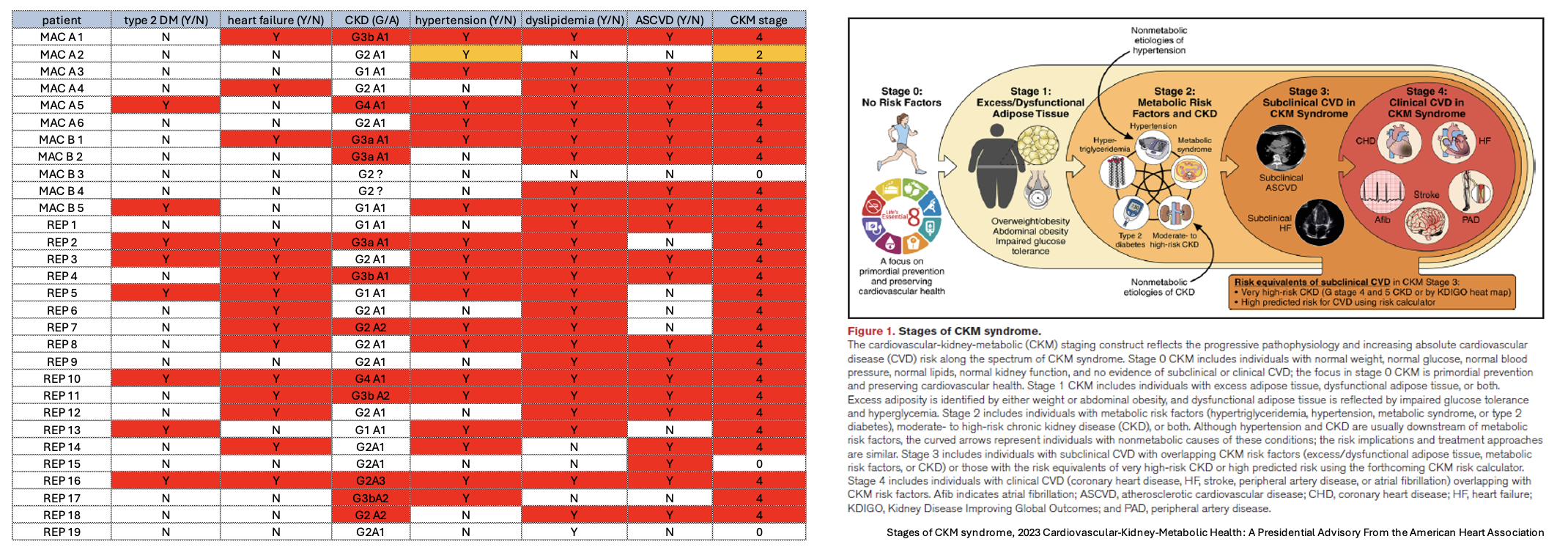
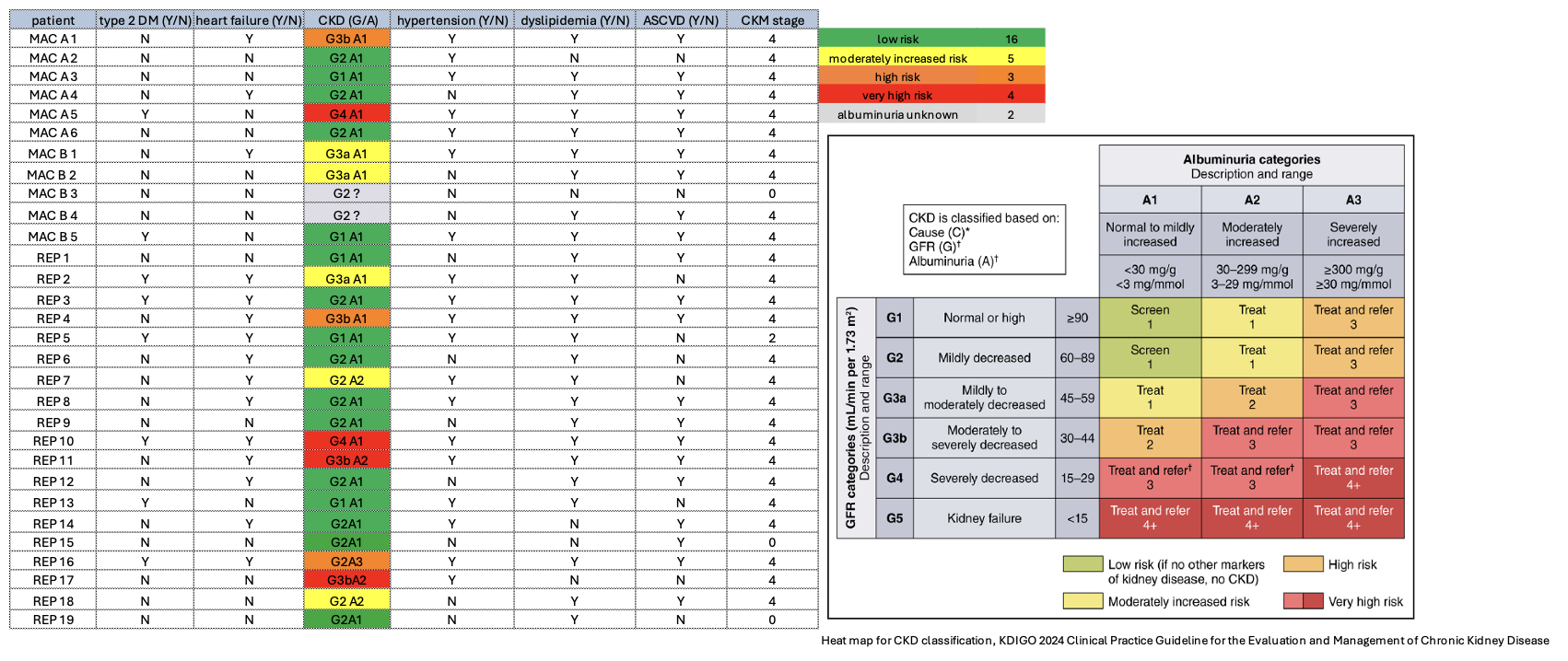
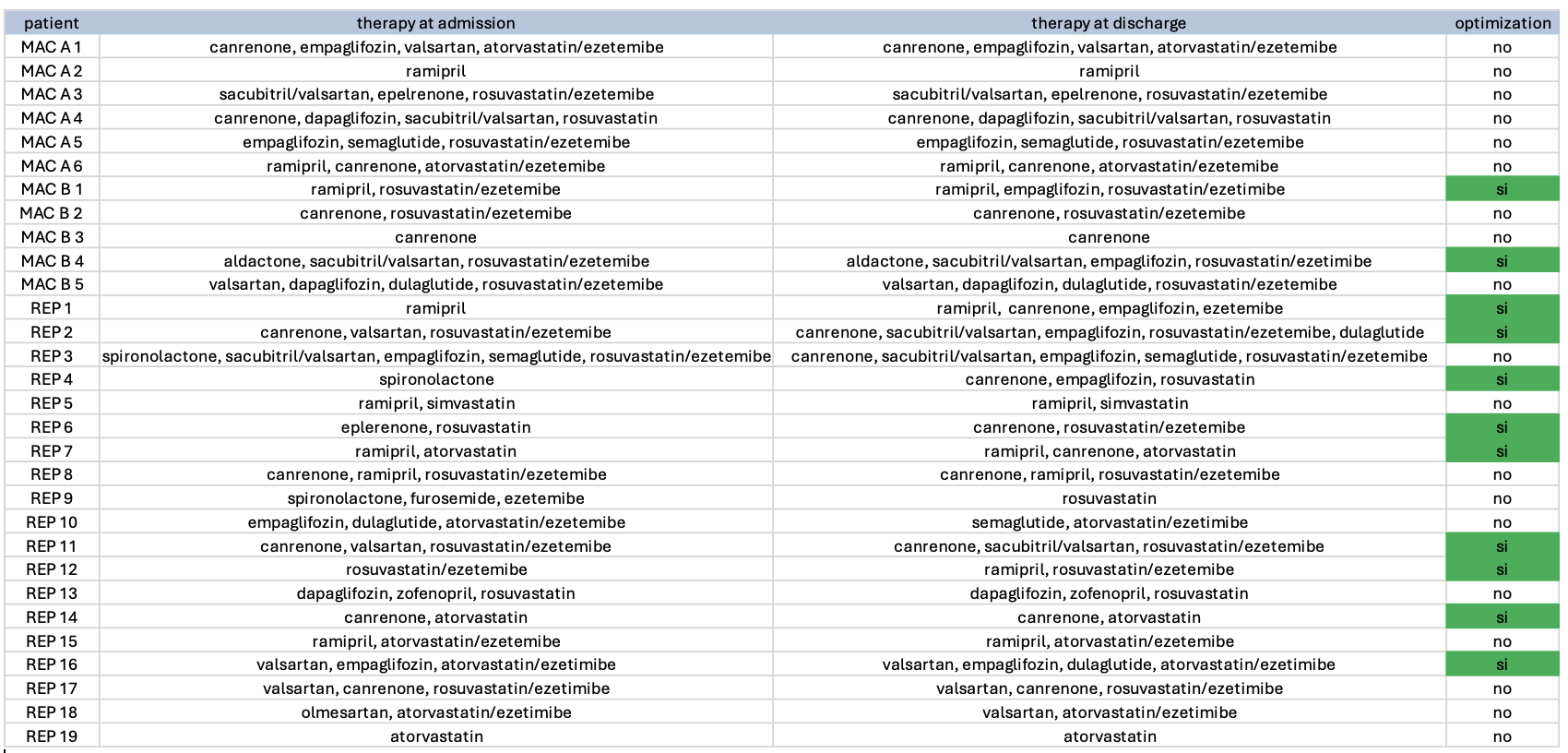
Background: Cardiovascular-Kidney-Metabolic Syndrome (CKM syndrome) is a clinical entity with major prognostic implications, characterized by a complex interrelationship between cardiac, renal, and metabolic dysfunctions, for which several therapeutic strategies have proven highly effective. While often associated with advanced chronic kidney disease (CKD), its prevalence in cardiac patients without severe renal impairment may be underestimated. The aim of this study was to evaluate the prevalence and severity of CKM syndrome, as well as the need for treatment optimization in a cohort of patients admitted to a Cardiac Rehabilitation Unit. Methods: We conducted an observational study on the 30 patients enrolled in a cardiac rehabilitation program at Carate Brianza Hospital (ASST Brianza) on a chosen day (September 24 th 2025), both as outpatients (MAC A/B) and inpatients (REP). Clinical and biochemical data were collected at admission, and pharmacological data at both admission and discharge. Patients were classified based on CKM syndrome stages, according to the 2023 American Heart Association presidential advisory, and CKD severity, according to the 2024 KDIGO classification. We focused of key drugs for CKM syndrome management: RAAS blockers, SGLT2 Inhibitors, GLP-1 agonists and cholesterol-lowering agents. Results: Out of the 30 patients, 26 (86.7%) presented with advanced CKM syndrome, ie. stage 4 (fig.1). Only 7 (23%) had moderate-to-severe CKD (fig.2). Metabolic and cardiovascular disorders were highly prevalent: type 2 diabetes was present in 8 (26.7%), heart failure in 15 (50%), hypertension in 19 (63.3%) and dyslipidemia in 25 (83.3%). During the rehabilitation program, a further optimization of CKD treatment was possible for 11 patients (36.7%) (fig.3). Conclusions: Our findings reveal a strikingly high prevalence of advanced CKM syndrome among cardiac rehabilitation patients, even in the absence of severe renal impairment, though the availability of spot urine albumin instead of urine albumin/creatinine ratio might have led to an underestimation of CKD severity. Despite most patients having been recently hospitalized in an acute care setting, therapeutic optimization was still possible in a significant percentage, underlying the central role of Cardiac Rehabilitation in managing cardiovascular, renal and metabolic dysfunctions. The high prevalence of stage 4 CKM syndrome at admission highlights the need for early multidisciplinary management.