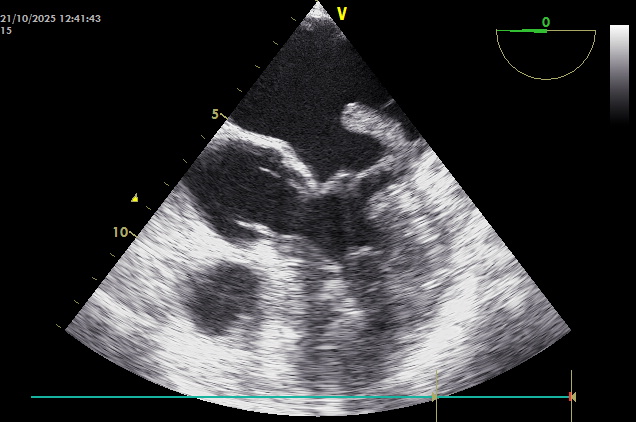
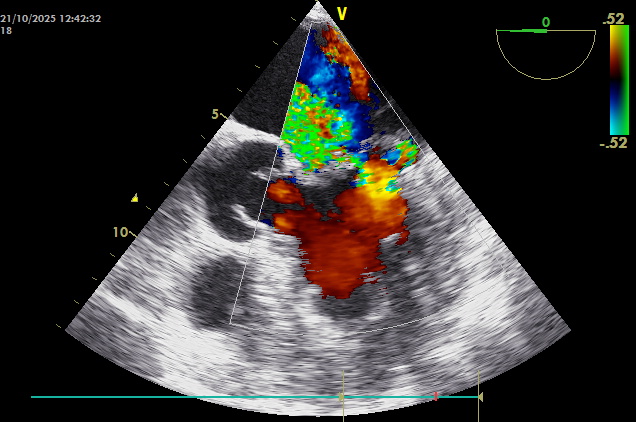
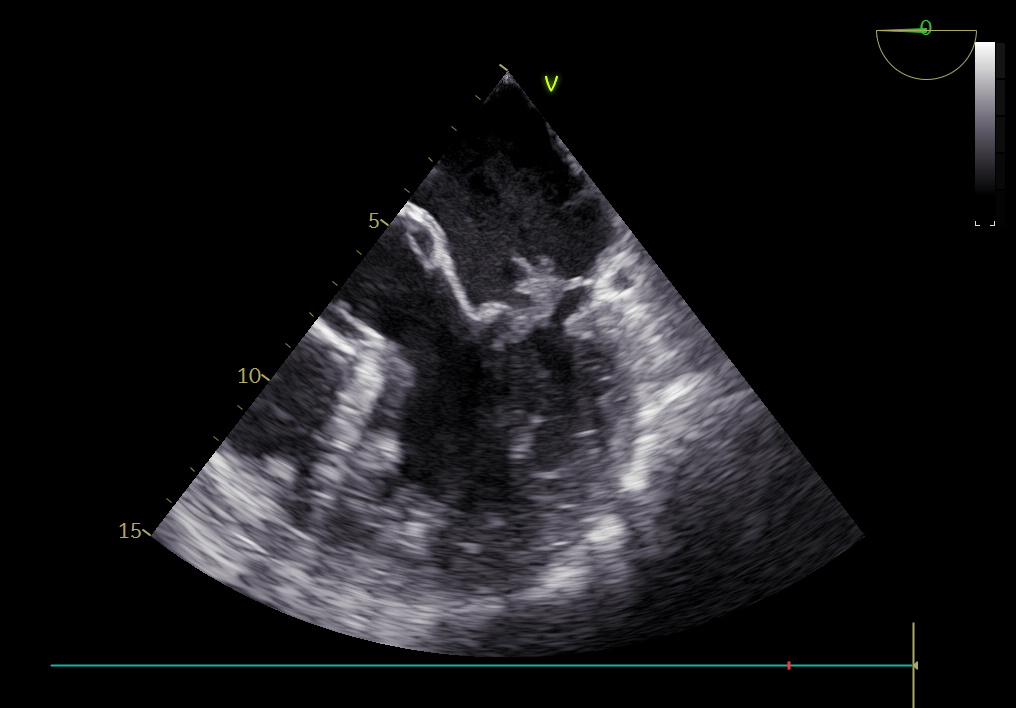
Introduction: The management of mitral infective endocarditis associated with large vegetations and embolic complications generally involves a combined medical and surgical approach. However, in selected cases, antibiotic therapy alone may lead to a favorable outcome. We report a case of significant regression of a mitral vegetation in a patient who did not undergo surgery due to refusal of the procedure. Case report: A 64-year-old man with paroxysmal atrial fibrillation and multiple sclerosis presented to our hospital with bilateral pleuritis in the setting of SARS-CoV-2 infection and a concomitant genitourinary infection. Blood cultures were positive for Escherichia coli . Transthoracic echocardiography revealed a vegetation attached to the posterior mitral leaflet (10 × 13 mm) associated with severe mitral regurgitation; transesophageal echocardiography confirmed the presence of a vegetative lesion measuring 26 × 12 mm (image 1) with severe valvular regurgitation (image 2). Total-body computed tomography and brain magnetic resonance imaging documented multiple lesions consistent with cerebral, splenic, and renal septic emboli. Despite a surgical indication, the patient refused cardiac surgery and therefore continued targeted antibiotic therapy until blood culture negativization. Follow-up echocardiography after one month showed a marked reduction of the vegetation to 9 × 8 mm (image 3), with mild-to-moderate mitral regurgitation. Discussion: Regression of the vegetation in the absence of surgery raises the hypothesis of a potential curative role of antibiotic therapy alone, possibly supported by ongoing anticoagulation. The lack of histological and microbiological confirmation of the valvular mass limits diagnostic certainty. Moreover, although the radiological findings were suggestive of septic emboli, the differential diagnosis remains broad, including sterile ischemic, neoplastic, and inflammatory conditions. Conclusions: This case suggests that, under selected clinical conditions and with careful monitoring, a conservative approach may represent a temporary or, rarely, definitive option in patients who are not surgical candidates or who decline surgery. Nevertheless, surgical intervention remains the standard of care in the presence of large vegetations and embolic complications.