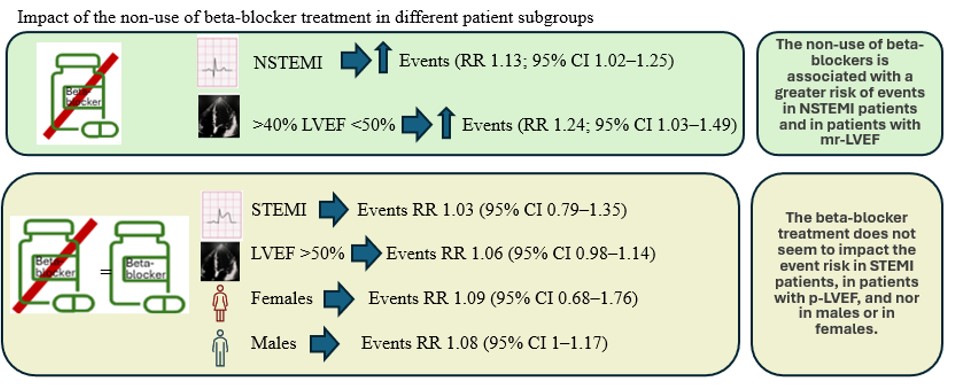
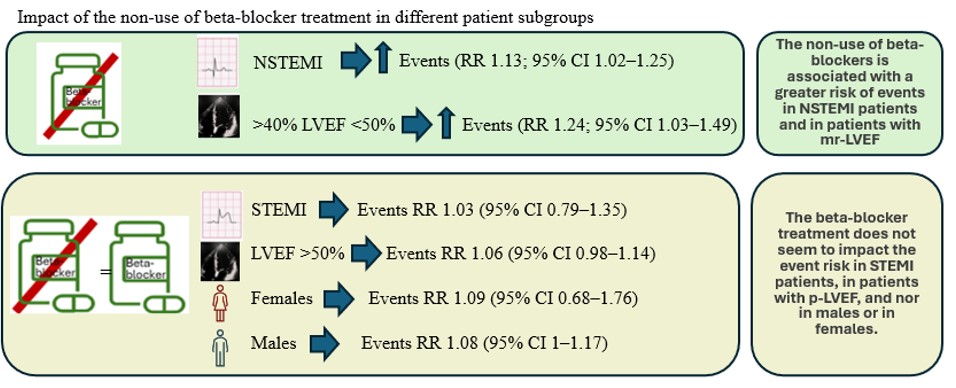
Background: The clinical benefit of beta-blocker treatment in patients with a previous myocardial infarction (MI) and without a reduced left ventricular ejection fraction (LVEF) is not established. This study aims at assessing the impact of beta-blocker treatment after an MI based on the type of MI at presentation, the LVEF, and the patient's sex in the setting of contemporary management of MI. Methods: We searched PubMed and Cochrane Library databases for randomized clinical trials reporting the impact on prognosis by MI type at presentation (with ST segment elevation, STMI, or without ST segment elevation, NSTEMI), LVEF, and sex (figure1). A meta-analysis was performed to assess the association between the non-use of beta-blockers and outcomes in different patient subgroups. Publication bias and small-study effects were assessed by funnel plots, with asymmetry tested using regression-based methods and corrected estimates explored via the trim-and-fill method. Results: The non-use of beta-blockers was found to be associated with a greater risk of adverse outcomes in NSTEMI patients (RR 1.13; 95% CI 1.02–1.25; I² 18%) and in patients with mildly reduced LVEF (RR 1.24; 95% CI 1.03–1.49; I² 0%) ( figure 2 ). No significant association between beta-blocker treatment and adverse outcomes was found in patients with a previous STEMI, in patients with preserved LVEF, in males and in females. Conclusions: Among patients with a previous MI and LVEF >40%, those not treated with beta-blockers seem to have a higher risk of adverse outcomes when the index event was a NSTEMI or when LVEF was mildly reduced.