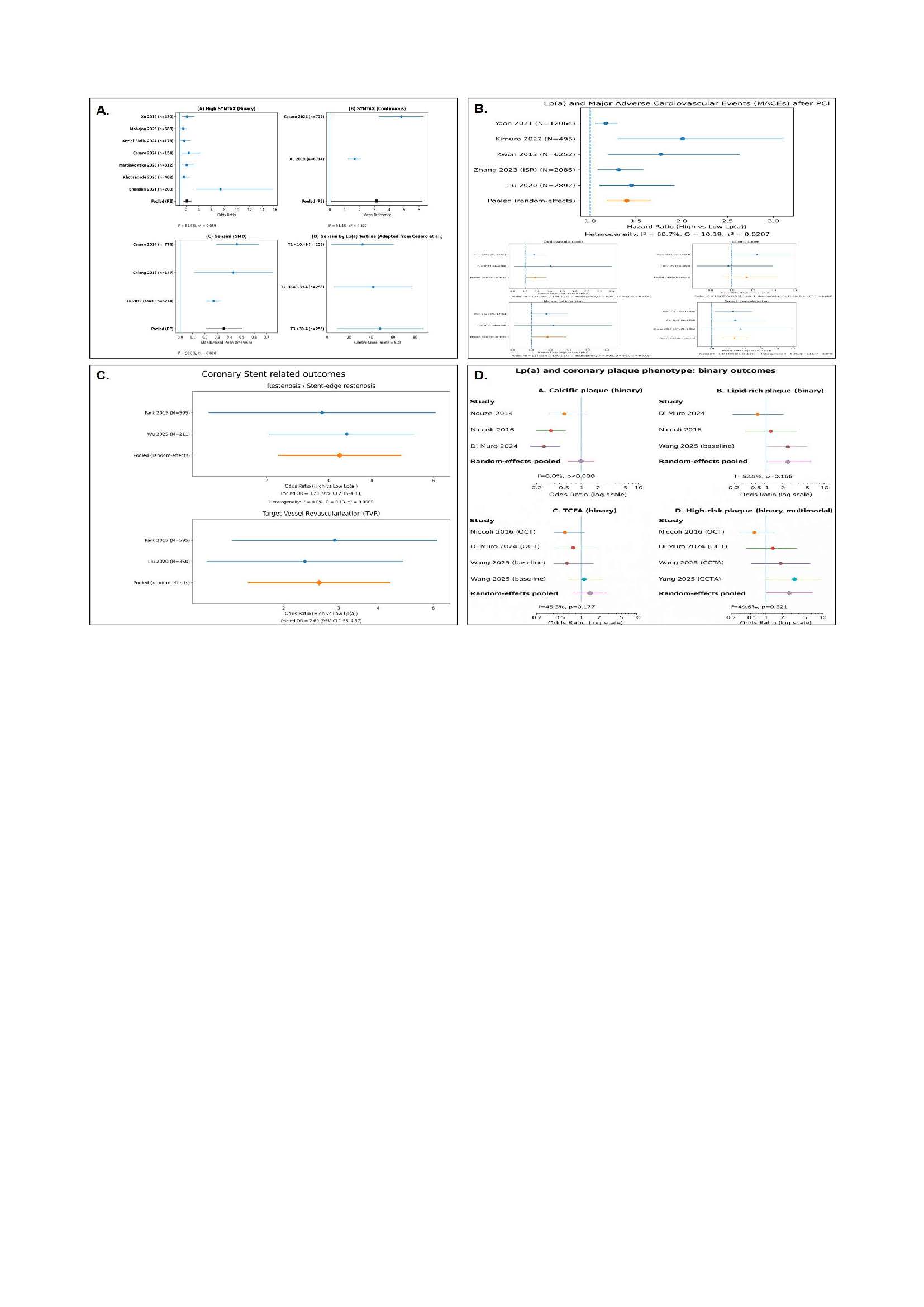
Background. Lipoprotein(a) [Lp(a)] is a genetically determined cardiovascular risk factor . However, its impact on coronary anatomy, plaque biology, and outcomes after percutaneous coronary intervention (PCI) remains incompletely defined from an interventional perspective. Methods. We performed a systematic review and random-effects meta-analysis of observational studies comparing high versus low Lp(a) levels in a pooled population of more than 40,000 patients . Prespecified outcomes included coronary anatomica! complexity (binary high SYNTAX, continuous SYNTAX, and Gensini score), major adverse cardiovascular events (MACE) after PCI, stent-related outcomes (in-stent and stent-edge restenosis, target vessel revascularization), and coronary plaque characteristics assessed by multimodality imaging (OCT, IVUS, CCTA) . Pooled estimates were derived using random-effects models . Results. Elevated Lp(a) was associated with greater coronary anatomica! complexity (pooled OR 1.5, 95% Cl 1 . 3- 1 . 6). High Lp(a) predicted worse post-PCI prognosis with higher MACE (pooled HR 1 . 5, 95% Cl 1 . 3- 1 . 7) . From a procedura! perspective, elevated Lp(a) significantly increased in-stent and stent-edge restenosis (OR 3 . 2, 95% Cl 2.2- 4 . 8) and the need far target vessel revascularization (OR 2 . 6, 95% Cl 1 . 6-4 .4) . Lp(a) was not associated with coronary calcific plaque but was significantly linked to vulnerable plaque phenotypes, including lipid-rich plaque and thin-cap fibroatheroma (high-risk plaque OR 2 . 1, 95% Cl 1.4- 3 . 1; TCFA OR 2.0, 95% Cl 1 . 3- 3 . 0) . Conclusions. Lp(a) bridges laboratory data and interventional decision-making, supporting a biologically infarmed approach that integrates anatomica! complexity, procedura! risk, and plaque vulnerability into PCI planning and fallow-up . These findings reinfarce the raie of Lp(a) as a key biomarker in advanced dyslipidemia and multimodality coronary imaging far personalized risk stratification .