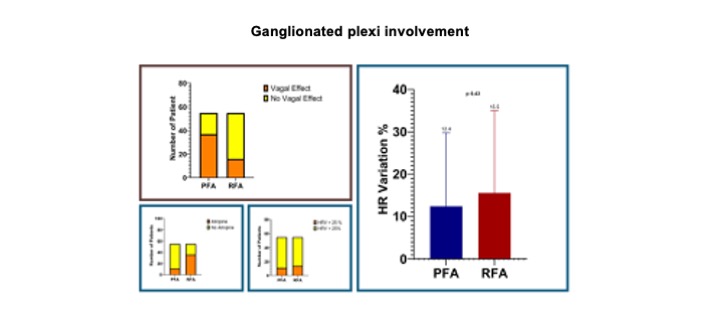
Background Pulsed field ablation (PFA) is a novel non-thermal ablative modality. Data about periprocedural time comparison between PFA and radiofrequency ablation (RFA) of atrial fibrillation (AF) are lacking. Purpose We would assess if PFA compared to RFA could have an impact on procedural organization and workflow of AF ablation, including effects on vagal nervous system. Methods In this retrospective, propensity-matched, case-control study we analyzed paroxysmal or persistent AF ablations, performed over the last year, 2024, in our high-volume center. In all cases only pulmonary veins isolation was performed. The population was divided into two groups: PFA group under deep sedation and RFA under light sedation. All procedures were supported by electro-anatomical mapping. We collected all procedural times as primary outcome, then we examined all other procedural data and vagal ganglionated plexi (GPs) involvement. Results This study included 110 patients (mean age 57±11,9, 61,8% males), 55 in PFA (mean age 58,1±8,7, 63,6% males) and 55 RFA group (mean age 55,9±14,3, 60% males). Baseline characteristics of patients are reported in fig.1. Longer post-procedural time (43,9±25,2 vs 19,3±8,3 min; p <0,001) was reported in PFA group. On the contrary, shorter skin to skin times (93,5±28,6 vs 131,9±35,2 min; p <0,001), mapping times (6,27±3,5 vs 13,1±4,1 min; p <0,001) and left atrium dwell times (45,6±8,6 vs 73,7±21,6 min; p <0,001) were evidenced for electroporation (fig. 2). No statistical differences were documented between PFA and RFA about pre-procedural (32±10,9 vs 28,1±6,8 min; p 0,96), ablation (22,2±7,5 vs 22,4±9,1 min; p 0,66) and total lab occupancy times (169,47±34,3 vs 179,4±35,2 min; p 0,05). Interestingly, fluoro-time was shorter in RFA (5,3±2,9 vs 3,3±3,2 min; p <0,001), but fluoro-dose was similar (15,3±17,2 vs 13±13,4 mGy/m 2 ; p 0,56) (fig.1 and 2). Complication rate was very low for both. About GPs involvement, heart rate variation before and after procedure was similar between PFA and RFA (fig.3). Interestingly, vagal reflexes were more frequently induced using PFA (67,2% vs 30,1%; p <0,001) and atropine use was more in RFA group (20% vs 65,4%; p <0,001). Conclusion PFA has a mild impact on periprocedural workflow using deep sedation protocol. There is no significant difference in total lab occupancy time when compared to RFA point-by-point ablation. Interestingly, more vagal reflexes were elicited in the PFA group.