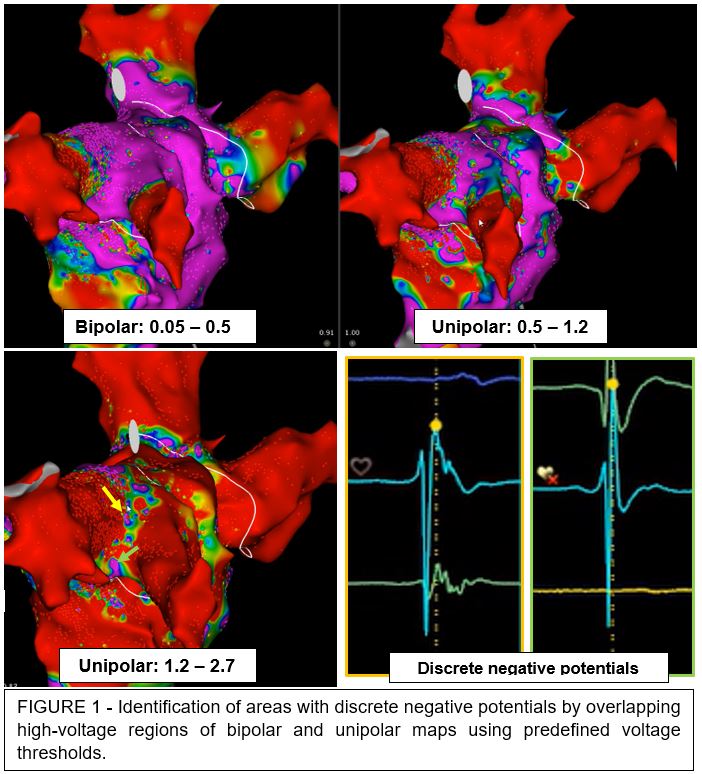
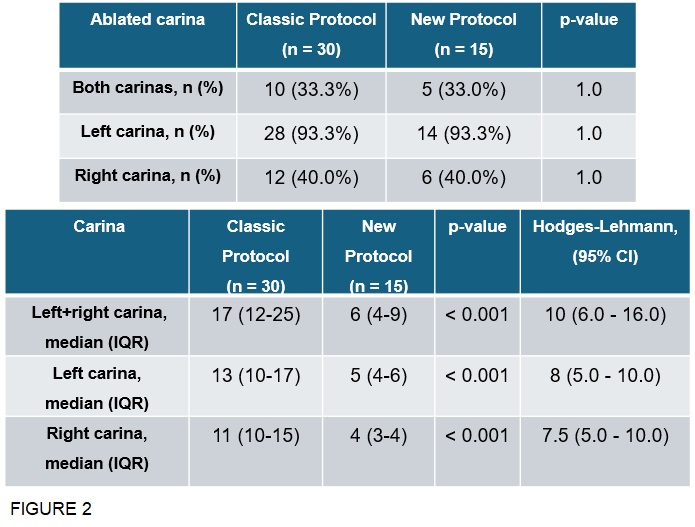
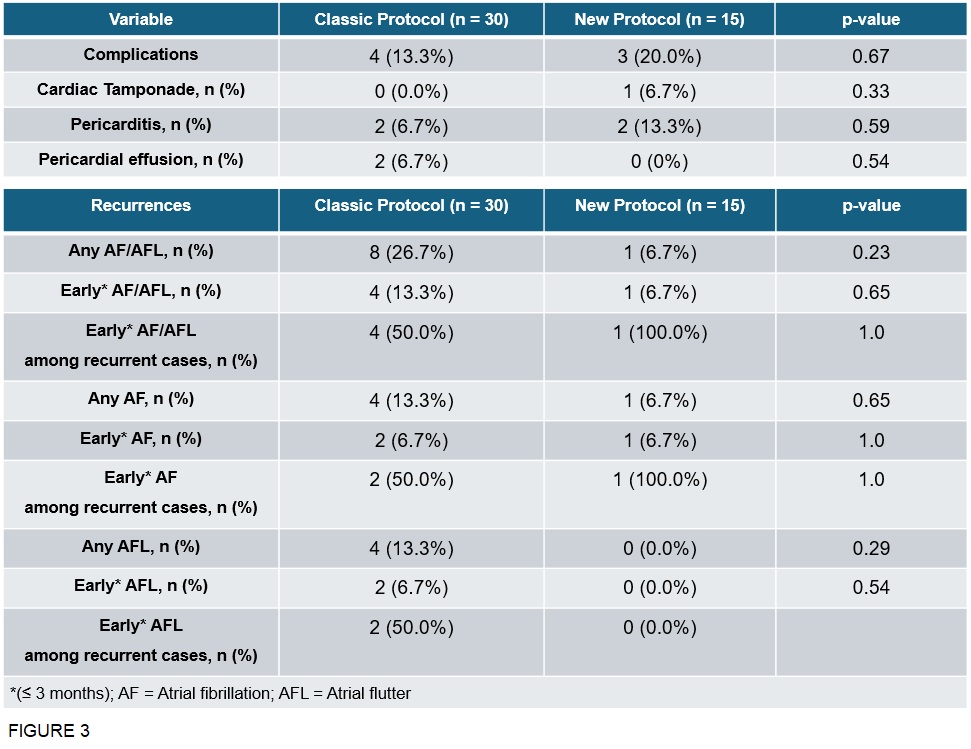
Background: Radiofrequency ablation (RFA) with pulmonary vein isolation (PVI) represents a cornerstone of atrial fibrillation (AF) treatment. Persistent conduction across the carina requires extensive additional ablation. Combining bipolar and unipolar voltage CARTO maps and applying voltage thresholds [Fig.1], our group observed areas with discrete negative potentials in the carina regions, which may represent critical sites for carina conduction. Objectives : The objective of the study was to evaluate whether selective ablation of discrete negative potentials (New Protocol, NP) within the carina could reduce the total number of radiofrequency applications required to achieve PVI compared with ablation of total carina extension (Classic Protocol, CP), without compromising safety or clinical efficacy. Materials and Methods: This single-center study included 45 patients undergoing RFA: 30 treated with the CP (July 2022 – April 2025) and 15 with the NP (April 2025 – October 2025). The evaluated outcomes included: number of ablation applications, periprocedural complications and arrhythmia recurrences [AF or atrial flutter (AFL)] during follow-up. Results: The population characteristics were comparable. The number of radiofrequency applications was significantly lower in the NP group [Total lesions, median: 6 vs 17; p < 0.001. Left carina, median: 5 vs 13; p < 0.001. Right carina, median: 4 vs 11; p < 0.001)] [Fig.2]. Complication rates showed no significant difference between groups (NP: 20.0%, CP: 13.3%; p = 0.67). Arrhythmia recurrences were analyzed with Kaplan-Meier curves; to ensure comparable observation a truncation of follow-up period (defined as period between ablation and end of follow-up or recurrence) at 6 months was performed and blanking period was excluded. A decreasing trend in recurrences was observed in the NP group, but with no statistically significant difference (p = 0.69) [Fig.3]. The greatest deviation between the curves was observed when only AFL recurrences in the first 6 months after ablation were considered, with no events in the NP group (p = 0.33). Conclusions: The New Protocol allowed to significantly reduces lesion burden without increasing procedural time or complication rates. Early observations regarding recurrence-free outcomes are promising though limited, due to a shorter follow-up and a smaller sample size in NP group. More definitive conclusions will require a longer follow-up and a higher number of patients.