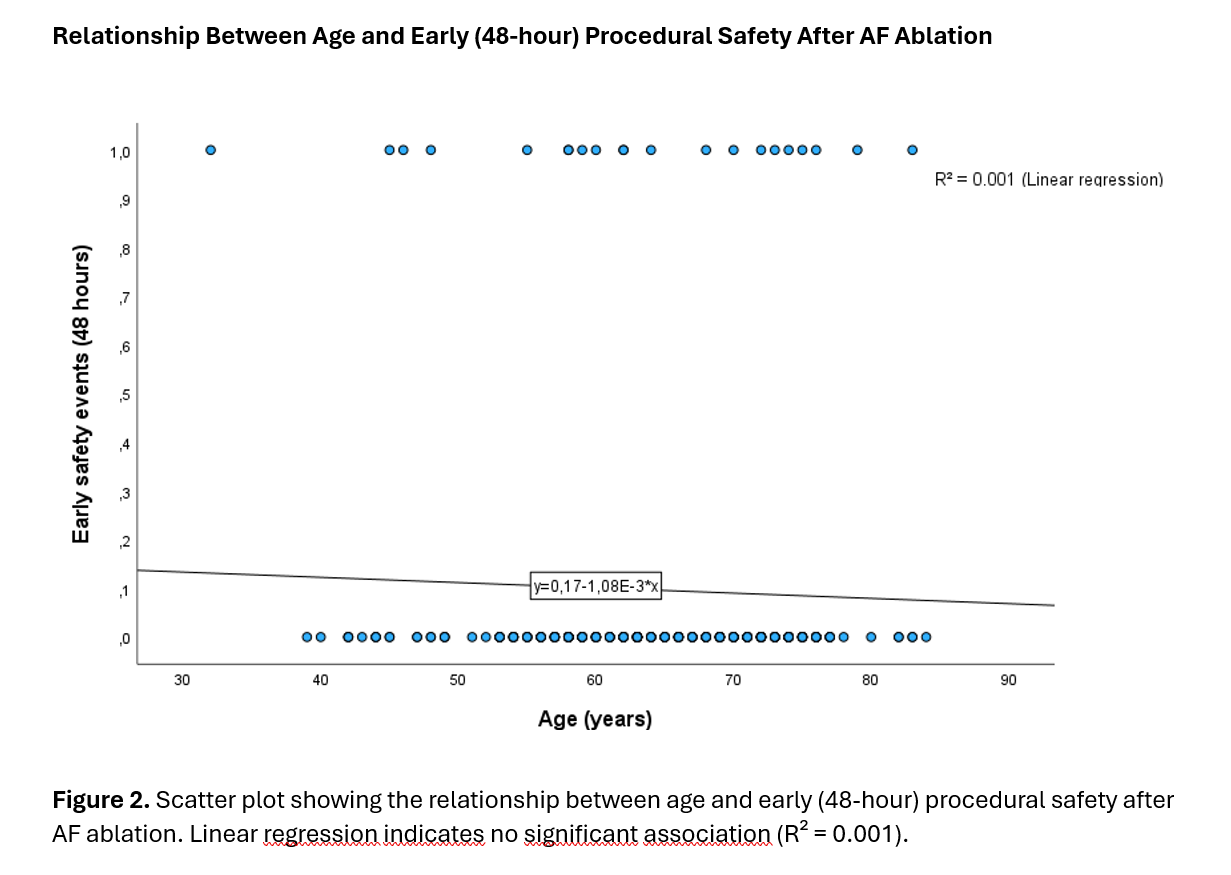
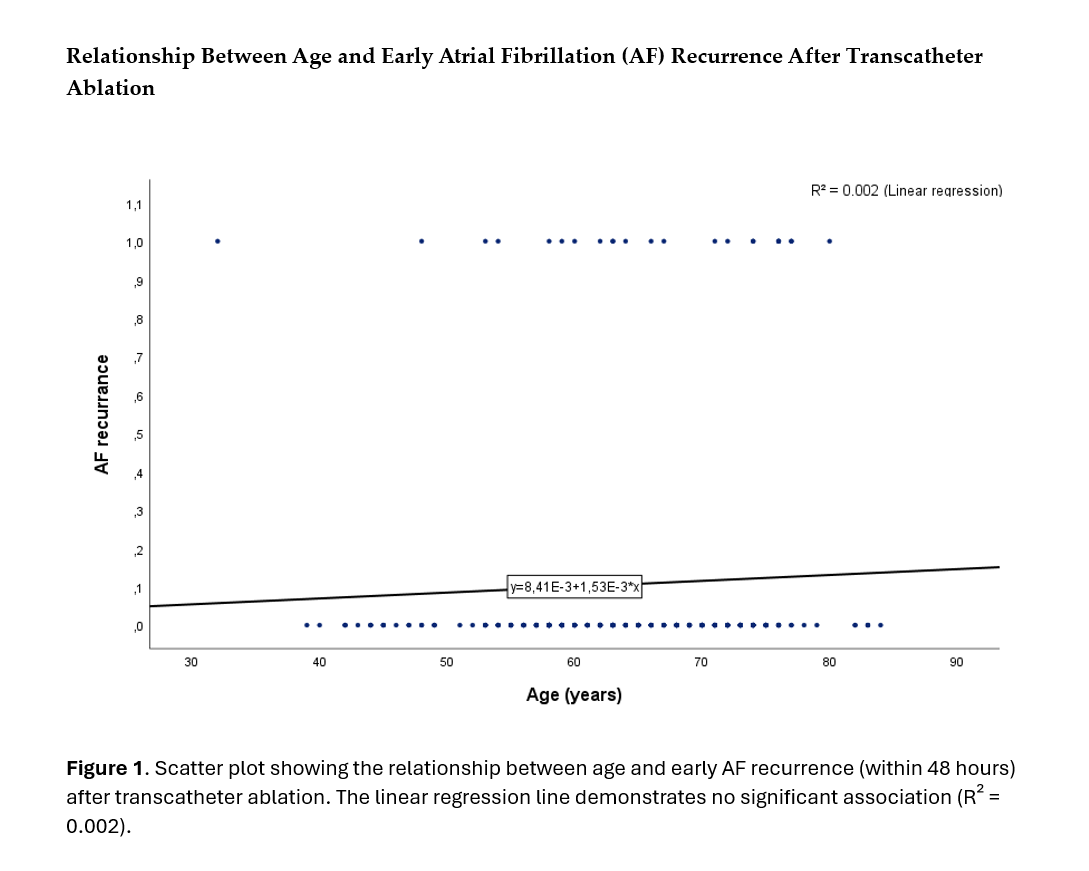
Background: Transcatheter ablation (TCA) is an established therapy for atrial fibrillation (AF), but the influence of age on procedural safety and early efficacy remains uncertain, especially in real-world practice. Objective: To determine the impact of age on early procedural safety and arrhythmic outcomes after TCA for AF in an unselected real-world cohort. Methods: We analyzed 217 patients (mean age 67 ± 9 years) who underwent TCA for AF at the Cardiology Unit of Ciriè Hospital (ASL Torino 4, Turin, Italy) between January 2022 and December 2023. Outcomes were assessed across three predefined age cutoffs (<65, <70, and <80 years) and with age modeled as a continuous variable. Logistic regression was used to evaluate the association between age and procedural safety and efficacy endpoints. Primary safety endpoints included a composite of pericardial effusion, pericardiocentesis, vascular complications, bleeding, stroke, and cardiovascular or all-cause death within 48 hours. Secondary efficacy endpoints consisted of a composite of AF recurrence and AF persistence within 48 hours, with both the composite and its individual components analyzed in covariate-adjusted models. Results: No significant differences in early complications or arrhythmic outcomes were observed across any age cutoff. In multivariable logistic regression, age was not independently associated with procedural safety (OR 0.98; 95% CI 0.93–1.03; p=0.69), AF recurrence (OR 1.01; 95% CI 0.97–1.05; p=0.77), or AF persistence (OR 1.00; 95% CI 0.96–1.05; p=0.91). Conclusions: In this real-world single-center cohort, age did not influence procedural safety or early arrhythmic outcomes after AF ablation. These findings indicate that advanced age alone should not preclude referral for TCA in appropriately selected patients.