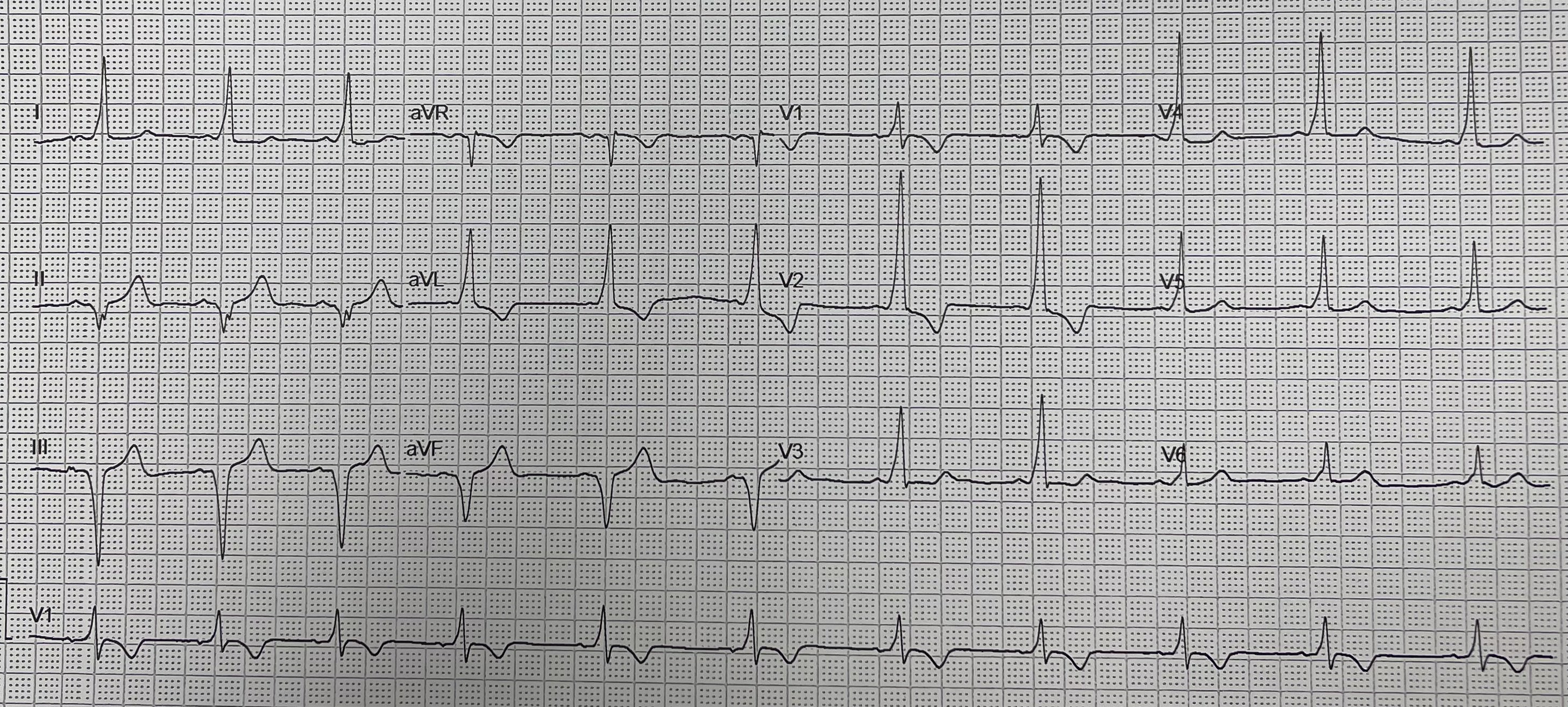
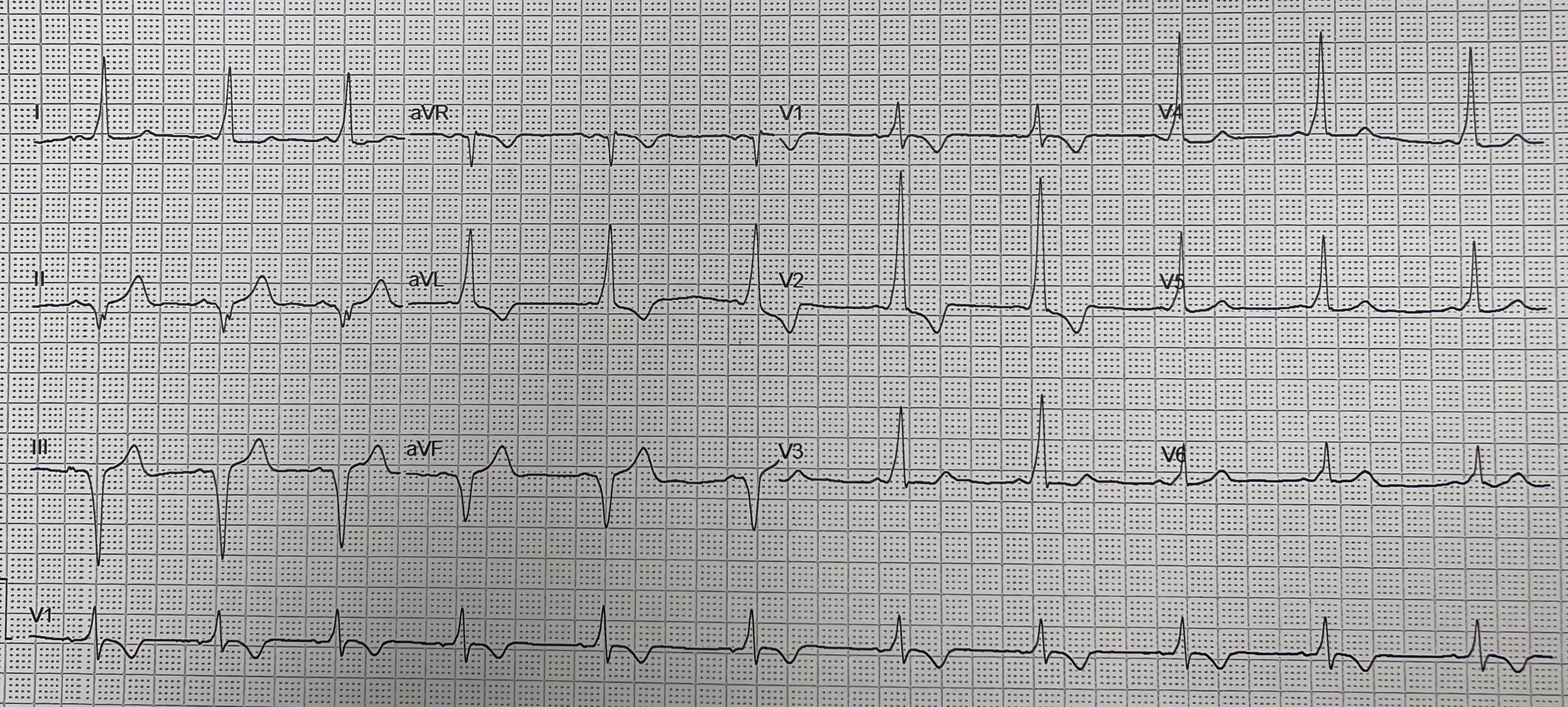
40-year-old male, no major cardiovascular risk factors, regular sports activity reported recurrent palpitations. In 2021, during excercise, he experienced palpitations associated with presyncope which resolved spontaneously, ECG revealed a short PR interval and delta wave, suggestive of a postero-septal accessory pathway. Exercise stress test induced a short episode of orthodromic tachycardia at 93% of the maximal predicted heart rate, spontaneously terminating. Electrophysiology study confirmed a postero-septal AP, although tachycardia was not inducible at that time. In 2023, due to increasing frequency of palpitations a second electrophysiology study was performed with the intention to ablate was planned. Programmed atrial stimulation induced AV re-entrant tachycardia with the earliest ventricular activation recorded on the CS 5–6 dipole, consistent with a postero-septal AP. Mapping of the left atrium via a patent foramen ovale identified a clear AP potential, preceding the QRS onset by 10–15 ms, between CS 5–6 and CS 7–8. However, several endocardial radiofrequency applications produced no effect on pre-excitation. Instead of proceeding to an epicardial puncture, intraluminal CS mapping was performed. Positioning the ablation catheter within the CS confirmed a sharp AP potential at CS 5–6, matching the earliest activation site. Radiofrequency ablation (15 W) was delivered from within the CS, resulting in abrupt loss of AP conduction after approximately 5 seconds. A full 40-second RF application was completed. No recurrence was observed after a 30-minute waiting period, and adenosine administration confirmed complete block of the accessory pathway. The patient was discharged the following day without complications. After more than 2 years of follow-up, the patient remains asymptomatic, shows no evidence of pre-excitation on serial ECGs, and reports full return to normal physical activity. Epicardial accessory pathways located along the postero-septal region can be technically challenging when approached endocardially. Because surface ECG cannot reliably distinguish endocardial from epicardial pathways, careful mapping within the coronary sinus is essential before considering epicardial access. Ablation from within the coronary sinus proved safe, effective, and avoided the need for percutaneous epicardial puncture. CS-guided epicardial ablation should be considered a valuable alternative when conventional endocardial ablation fails.