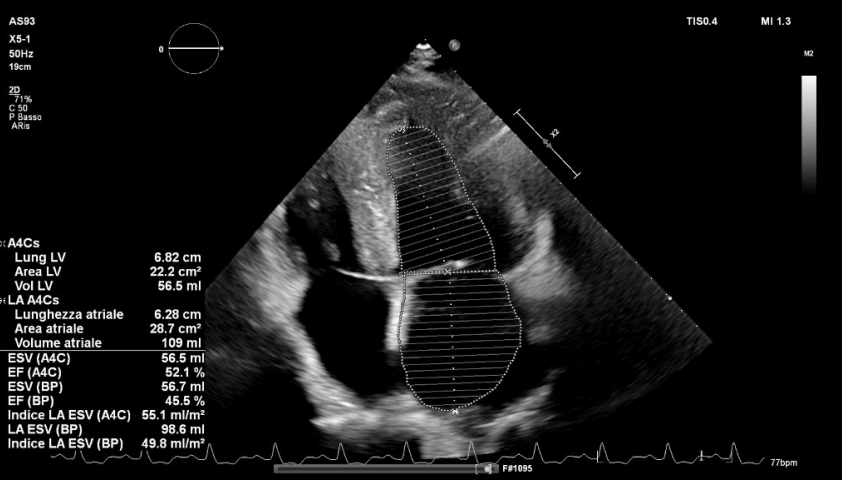
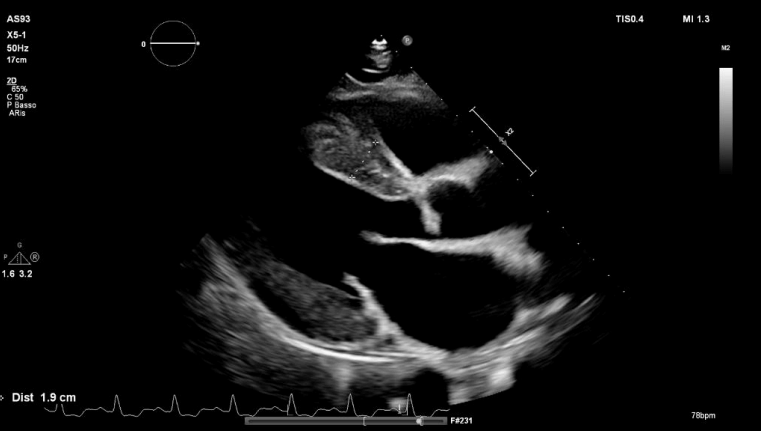
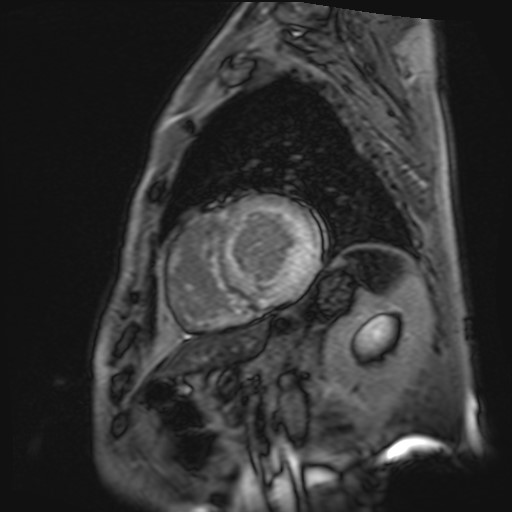
Wild-Type Transthyretin Amyloidosis (ATTRwt) is a progressive infiltrative cardiomyopathy, often preceded by typical extracardiac manifestations that can serve as early diagnostic red flags. While the cardiac phenotype is carachterised by concentric hypertrophy and is thus restrictive, management is frequently complicated by hemodynamic fragility that limits the use of standard heart failure therapies. We report the case of a 74-year-old man with a revealing history of bilateral carpal tunnel syndrome and of trigger finger syndrome. After a prolonged preclinical phase, the clinical scenario rapidly evolved: he presented with paroxysmal atrial fibrillation, rate-dependent left bundle branch block, and sudden overt heart failure symptoms (NYHA class II) with an ejection fraction declining to 46%. Transthoracic echocardiography showed severe concentric left ventricular hypertrophy (IVS 19 mm), pathognomonic apical sparing and granular sparkling. Cardiac Magnetic Resonance (CMR) confirmed the diagnosis (IVS 23 mm, extensive diffuse LGE, ECV 52%). DPD scintigraphy showed a Perugini score of 3, while genetic testing excluded TTR variants, thus confirming ATTRwt. Pharmacological management proved challenging due to hemodynamic fragility: significant hypotension required suspension of angiotensin receptor blockers and of loop diuretics. Disease-modifying therapy with Tafamidis was initiated alongside an SGLT2i (Dapagliflozin), later interrupted for a relapsing fungal infection. Strict cardiovascular risk factor control was implemented (non-critical coronary atherosclerosis on Cardiac CT). This case highlights a specific trajectory of ATTRwt characterized by a prolonged period of clinical quiescence, where orthopedic history provided red flags, followed by a rapid onset of the cardiac manifestations. We also aim to highlight the complex therapeutic balance required in these patients: standard heart failure therapy is often poorly tolerated due to hemodynamic fragility, necessitating an approach focused on disease-modifying agents.